Porphyrias with cutaneous findings Flashcards
What is the mainstay of treatment for porphyrias?
diligent photoprotection with physical sunblock, avoidance of skin trauma and good skin care
What is the most common porphyria?
PCT
PCT is due to:
decreased hepatic uroporphyrinogen decarboxylase (UROD) acticity
What is the most common form of PCT?
acquired/sporadic
What are the skin findings seen in PCT?
In photo distribution:
- vesicles
- bullae
- erosions
-milia
-scarring
- hyperpigmentation
- hypertrichosis
(classic pic is hemorrhagic blisters on dorsal hands)

What is the pathogenesis of PCT?
What are the associations/triggers in PCT?
- alcohol abuse, estrogen, hemochromatosis, hep C, HIV
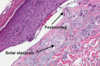
What is histology of PCT?
cell-poor subepidermal bulla w/ “festooning” of dermal papillae, “caterpillar bodies” (pink BMZ material in blister cavity and epidermis
- festooning epidermis is due to fibrosis that allows dermis to stay in tact within blister
DIF findings of PCT?
IgG, IgM, fibrinogen, and C3 linearly along BMZ and in superficial dermal vessels (see thickened deposits around vessels)
Tx of PCT?
avoid precipitating factors! (sunlight, alcohol, estrogen)
- phlebotomy for hemochromatosis
- low dose plaquenil and deferasirox
X-linked dominant protoporphyria is due to ____mutation
gain of function ALAS2 gene that encodes 5-ALA
Hepatoerythropoietic porphyria is due to (heterozygous/homozygous) mutation of ______
homozygous mutation of uroporphyrinogen decarboxylase (UROD)
Hepatoerythropoietic porphyria starts at what age?
childhood/infancy
Hepatoerythropoietic porphyria presents with what skin findings?
- scarring, sclerodermoid changes, photosensitivity to point of mutilation, hypertrichosis, milia, vesicles,
Variegate porphyria is due to mutation of
protophrphyrinogen oxidase
