Physiology Review Q's Flashcards
1. Physiology humoral and nonhumoral factors (1-26) 2. seminar arterial pulse (27-69) 3. cardiac muscle action potentials (70-129) ---- 4.ECG seminar 1 (130-149) 5. ECG seminar 2 (150-165) 7. pathophysiology of arrhythmias (166-185) 8. cardiac cycle (186-216) 9. regulation of cardiac volume (217-252) 10. regulation of contraction of cardiac muscle (253-292) 11. regulation of cardiac output (293-322)
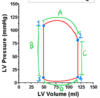
Describe the relationship between blood pressure and volume?
a. directly proportional
b. inversely proportional
a. directly proportional
Where are two locations that arterial baroreceptors are found?
aortic arch and carotid sinus (the wider area before the internal carotid artery splits)
What two nerves are the afferent pathway of baroreceptors?
CN X and IX
(CN X for the aortic arch and CN IX for the carotid sinus)
Describe action potentials of baroreceptors during low pressure vs high pressure?
more firing during high pressure and less during low pressure
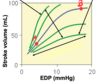
Describe the relationship between compliance and pressure
inversely proportional
During low blood pressure, how will baroreceptors act on vasopressin, sympathetic, and parasympathetic activity?
increase vasopressin
increase sympathetic activity
decrease parasympathetic activity
What is the effect of the setpoint atrial blood pressure on sympathetic activity?
ABP at setpoint inhibits sympathetic activity
During high blood pressure, how will baroreceptors act on vasopressin, sympathetic, and parasympathetic activity?
decrease vasopressin
decrease sympathetic activity
increase parasympathetic activity
Which body reflex prevents pulmonary edema?
the atrial mechanoreceptor reflex
(AKA Bainbridge reflex or cardiopulmonary reflex)
During pulmonary congestion, how will baroreceptors act on vasopressin, sympathetic, and parasympathetic activity?
decrease vasopressin
increase sympathetic activity
decrease parasympathetic activity
(Atrial mechanoreceptor reflex)
In which of the following can tachycardia be found? explain.
a. brain ischemic reflex
b. cushing reflex
a. brain ischemic reflex
(this reflex is associated with hypotension, so the tachycardia is used to compensate; the cushing reflex has hypertension, so the baroreceptor reflex is used to compensate)
Which (one or more) of the following inhibits parasympathetic/ vagal activity?
a. brain ischemic reflex
b. crushing reflex
c. baroreceptor reflex
d. atrial mechanoreceptor reflex
e. atrial chemoreceptor reflex
d. atrial mechanoreceptor reflex
AKA bainbridge reflex
Which of the following is both sympathetic and parasympathetic activity activated?
a. brain ischemic reflex
b. crushing reflex
c. baroreceptor reflex
d. bainbridge reflex
e. atrial chemoreceptor reflex
e. atrial chemoreceptor reflex
How does angiotensin 2 affect blood pressure? explain.
it increases BP by vasoconstriction and helping release aldosterone and vasopressin/ADH which then reabsorb Na and water
(it also indirectly enhances sympathetic activity by increasing NA release and by increasing reactivity to adrenergic stimulation)
How do ANP and BNP affect BP and how?
(atrial natriuretic peptide (ANP); B-type natriuretic peptide (BNP))
decrease BP by promoting vasodilation and natriuresis
What degrades natriuretic peptides?
Neprilysin
What is used as a biomarker of heart failure? Why?
proteolytic fragments of B-type natriuretic peptide (BNP)
(WHY? Natriuretic Peptides are high in heart failure. They’re r_eleased when the atrial pressure is high_ and its dilated, they act to reduce the BP- by natriuresis= the excretion of sodium by the kidneys)
How can we reduce mortality in heart failure patients?
sacubitril (neprilysin inhibitor) and valsartan (angiotension II receptor blocker)
** this combo is called ARNI
Which of the following does vasopressin use to increase systemic vascular resistance?
a. cAMP
b. IP3
b. IP3
(vasopressin uses cAMP to increase blood volume)
Which cells produce nitric oxide? What stimulates their synthesis?
endothelial cells; blood flow shearing forces and NO-dependent vasodilators stimulate synthesis.
What is a potential issue that may develop after endothelial destruction?
Atherosclerosis
Give me four vasodilators/activators of NO synthase.
Acetylcholine (usually)
Adenosine
Bradykinin
Substance-P
When does acetylcholine do vasoconstriction/dilation?
causes constriction when directly related to vascular smooth muscle
causes dilation when endothelium present
Which second messenger does NO use to mediate vasodilation?
cGMP