What are the AIDS-defining cancers?
Kaposi sarcoma, Lymphoma, Cervical SSC
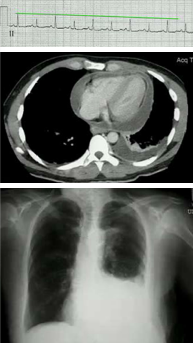
A 68 year old patient with HIV has CD4 count of 100 and a viral load of 100. He has had HIV for 30 years. He has the skin lesion below, chronic cough and fatigue. His peripheral blood smear and CXR are shown below. What is causing his symptoms?
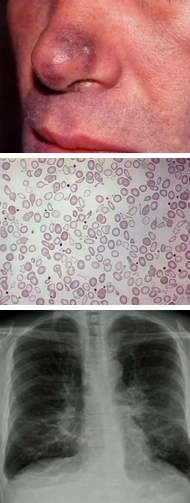
Visceral Kaposi sarcoma in the GI and respiratory tracts. Note the hypochromatic RBCs indicating iron-deficiency anemia from GI blood loss.

3 subsets of Kaposi sarcoma
1) Sporadic (Mediterranean men) 2) Epidemic (HIV infection) 3) Endemic sub-Saharan Africa unrelated to HIV (Lymphadenopathic and cutaneous subtypes)
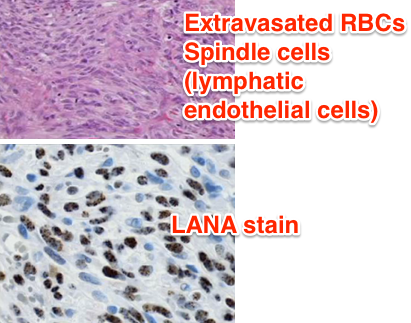
Causative agent of Kaposi sarcoma? How do you make a definitive diagnosis?
DNA virus HHV-8 is present in 100% of Kaposi sarcomas. You need to biopsy to differentiate from bacillary angiomatosis.
How is HHV-8 spread?
Saliva
How are the majority of spindle cells in Kaposi sarcoma infected? What proteins do they produce?
Latently infected: LANA-1 inhibits p53 and induces angiogenesis. vCyclin blocks cdk inhibitors (p21 and p27) and induces cell cycle entry. vFLIP: inhibits apoptosis. Note that malignant transformations ors not occur in latently infected cells, only lytic cells.
1st line therapy for Kaposi sarcoma
ART. This prevents loss of CD4 T-cells that improves CD8+, NK cell and B-cell response to infected cells. Additionally reducing viral load reduces the inflammatory state and cytokine release that upregulates receptors on endothelial cells which allows for more uptake of virus.
Therapy for lytic Kaposi sarcoma
Liposomal adriamycin (doxorubicin).
A man with HIV presents with an upper duodenal mass. Biopsy is shown below. What is your diagnosis?
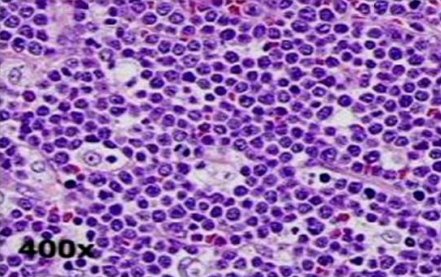
“Starry sky” = Burkitt lymphoma
3 types of AIDS defining lymphomas
Peripheral, primary CNS and primary effusion lymphomas.
Lymphomas in patients with HIV that are often associated with EBV?
Burkitt endemic (100%), Diffuse large B cell immunoblastic (100%), Burkitt epidemic (30%), Diffuse large B cell centroblastic (30%). Note that centroblastic has a better prognosis.
Tx for HIV patients with peripheral lymphomas
EPOCH: Etoposide, Prednisone, Vincristine (Oncovin), Cyclophosphamide, Doxorubicin (Hydroxydaunorubicin). All patient get CNS prophylaxis with MTX or cytosine arabinase. Stop ARTs b/c of drug interactions.
A 59 year old long-standing HIV patient presents with a CNS lesion. CD4 count is
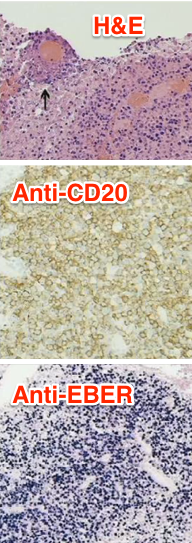
Diffuse Large B Cell Immunoblastic Lymphomas are the most common cause of primary CNS lymphoma in patients with HIV. These are always EBV+ and have a poor prognosis. Tx with ARTs, radiation, high dose MTX w/leucovorin rescue, temozolomide and rituximab (Anti-CD20) followed by ARA-C with etoposide.
A 26 year old HIV patient presents with progressive dyspnea. RR 35, P 125, BP 103/60 w/pulsus paradoxus of 25 mmHg on inspiration. Labs show electrical alternans, pericardial/pleural effusions. Biopsy reveals B-cells that are LANA positive. What is causing his condition and how do you treat it?
Primary effusion lymphoma is caused by KSHV infection of B cells. There is never a solid mass, it is usually confined to the pericardium, pleura and peritoneal cavity. They are CD20 negative so rituximab won’t work and the tumor is refractory to chemotherapy so prognosis is very poor (
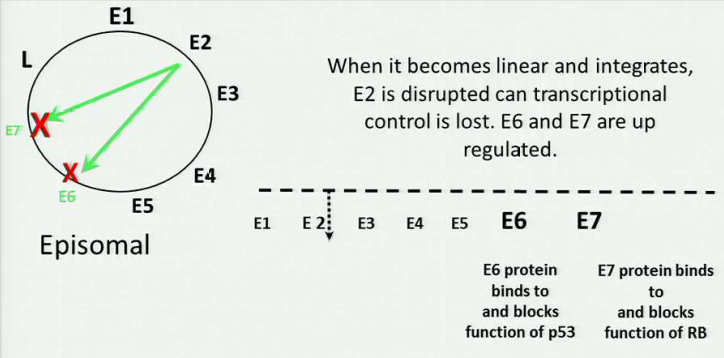
A 32 year old HIV patient has HPV infection and CIN II. Why is she at high risk for cervical carcinoma?
When cellular and humoral immunity are compromised, HPV is persistent and is more likely to go from an episomal DNA to DNA integrated with the host cell (because loss of E2 = expression of E6 and E7 block p53 and Rb respectively)
Tx for invasive cervical cancer
Radiation, surgery and chemotherapy
A 44 year old HIV patient presents with vertigo, dysarthria and difficulty walking. CT shows enlarged hilar lymph nodes and biopsy reveals lung adenocarcinoma. What is causing his condition?

HIV patients are at higher risk for lung cancer because of chronic inflammation and decreased CD4 surveillance.
-
Path Lab-Trauma92
-
Multisystems I - First Aid230
-
Microbiology-Vaccine Preventable Bacterial Diseases of Childhood22
-
Microbiology-Viral Diseases of Childhood41
-
Prev Med-Vaccine Safety10
-
Prev Med-Services for Adults24
-
Pathology-Forensic Pathology24
-
Pathology-Environmental Disease12
-
Prev Med-Environmental Health12
-
Prev Med-Occupational Health14
-
Immunology-Response to Infection30
-
Immunology-Hypersensitivity Reactions15
-
Pharmacology-Hypersensitivity Intervention14
-
Immunology-Accepting, Rejecting, Replacing Self31
-
Pathology-SLE42
-
Pathology-RA and Scleroderma24
-
Pharmacology-Immunomodulators52
-
Pharmacology-Antibiotics150
-
Pathology-Multisystems Disease36
-
Pharmacology-Antibiotic Resistance13
-
Immunology-Primary Immunodeficiency16
-
Microbiology-HIV Virology21
-
Pharmacology-Antiviral Tx28
-
Pharmacology-HIV Care17
-
Preventive Medicine-Health Disparities7
-
Pharmacology-ART Guidelines29
-
Pathology-Metabolic Effects of HIV15
-
Pathology-AIDS-related Malignancies17
-
Microbiology-Opportunistic Mycoses35
-
Microbiology-Opportunistic Infections33
-
Preventive Medicine-Prevention & Communication13
-
Path Lab-Infectious Diseases I87
-
Physiology-Cancer Survivorship23
-
Physiology-Death17
-
Physiology-Diabetes12
-
Physiology-Geriatrics24
