Pathology Flashcards
Placenta: Umbilical Cord
2 Arteries & 1 Vein

Placenta: Codyledins
Anchors into endometrium– look to see if they are intact after delivery, if torn– parts of codyledin are left behind and can cause maternal bleeding.
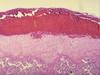
Placenta 1st trimester
edematous chorionic vili, few syncytial knots, sparse vasculature, stroma separated by 2layers—outer syncytiotrophoblast & inner cytotrophoblast

Placenta 2nd Trimester
More vessels w/in chorionic villi, more syncytial knots, some fibrin (too much is path), less edematous, more cellular

Placenta: 3rd Trimester
small villi, w/ more vessels, thinned syncytio/cytotrophoblast

Spontaneous Abortion
<20wks—most are <12wks
Fetal Cause: CHROMOSOMAL abnormalities
Maternal Cause: luteal phase defect, uncontrolled diabetes or endocrine disorder, uterine defect—polyps, leiomyomas, malform,
*Listeria*, Toxo, Mycoplasma or viral
Ectopic Pregnancy
≈90% in Fallopian Tubes—*PID –> tube scarring*
MOST common cause of HEMATOSALPINX
NO decidual cells in tube for proper invasion/attachment/growth
Tube rupture–>massive intraperitoneal hemorrhage
Late Pregnancy Disorders
Constricting KNOTS or cord compression
True Knot vs. False Knot
true can be reduced
false can NOT be reduced
Cord Coiling
Degree of fetal activity and implantation site –higher placenta -> more twisting
Abruptio Placenta
RETROplacental hemorrhage, intravillous fibrin deposition
Other Late Pregnancy Disorders
Uteroplacental malperfusion, maternal vascular disease–preeclampsia, uteroplacental ischemia, IUGR
Placenta Acreta
Placenta attaches into myometrium–villi invade

Twin Placenta
Diamnionic Dichorionic
Diamnionic Monochorionic
Monamnionic monochorionic
If placental is fused look to see how many amniotic sacs there are.
Diamniontic: Amnion on boths sides of chorion
Twin-Twin Transfusion Syndrome:
monochorionic, vascular anastomoses that connects the twins’
circulation—1 twin gets better blood supply, death to 1 or both
Infections
Think BACTERIA!
Ascending Infection: Bacterial, Cloudy amniotic fluid w/ purulent exudate, neutrophils at chorion-amnion interface, vasculitis,
FUNICITIS—Wharton’s Jelly infected
Hematogenous: Acute VILLITIS—infection
along chorionic villi
TORCH
Toxoplasmosis, Other, Rubella, CMV, HSV—
CHRONIC inflammatory infilitrates in chorionic villi, LYMPHOCYTIC infiltrate
Preeclampsia

*HTN, Edema, & Proteinuria (>0.3)*f—LAST trimester
HTN caused by rxn to sperm
Eclampsia—convulsions
↑syncytial knots, accelerated vilous maturity, placental infarcts, ↑retroplacental hematomas, *fibrinoid necrosis* or atherosis of decidual vessels, liver lesions—hemorrhagic necrosis, kidney
lesions—mesangial hyperplasia, fibrin in glomeruli, brain hemorrhage
Hydatidiform Mole
Cystic swelling of chorionic villi, variable trophoblastic proliferation, *↑risk of persistent invasive mole or choriocarcinoma*
Higher risk at Beginning & End of reproductive years
**Ovum LACKING MATERNAL chromosomes—PATERNAL 46 XX**
Androgenesis: 1 sperm duplicates genome
Complete Mole
**Grape-like, swollen mass of chorionic villi**
Enlarged edematous viili & *Diffuse Trophoblast Hyperplasia*
Partial Mole

Egg fertilized by 2 haploid PATERNAL chromosomes—DISPERMY *69 XXY*, maternal chromosomes PRESENT
Less edematous villi & trophoblastic proliferation
*NOT ↑ risk of choriocarcinoma but ↑risk of persistent molar dz*
Invasive Mole

**MYOMETRIUM invasion by hydropic chorionic villi—proliferation of BOTH cyto- & syncytiotrophoblast**
Hyropic Villi—EMBOLIZE to lungs & brain
*Persistently ↑serum HCG*, vaginal bleeding, irregular uterine enlargement,
varying degrees of ovarian luteinization, responds well to chemo
Choriocarcinoma

**Malignant TROPHOBLASTIC cells**
Does NOT produce chorionic villi, mixed proliferation of BOTH cyto- & syncytiotrophoblasts, lots of mitoses, invades myometrium, vessesl, lymphatics, etc,
from normal, abnl, ectopic pregnancy—retained tissue
RAPIDLY invasive, widely metastatic, respond well to chemo
*ISCHEMIC NECROSIS*, focal cystic softening,
extensive hemorrhage
Mets to: lungs, brain, bone marrow, liver & others
Placental- Site Trophoblastic Tumor

**Neoplastic proliferation of EXTRAVILLOUS TROPHOBLASTS**
aka Intermediate Trophoblast
**Cyto- & Syncytiotrophoblasts on chorionic villi**—infiltrate ENDOMETRIRUM
50% preceded by NORMAL pregnancy—GOOD prognosis if localized
or <1yr to dx
