MSK/Ortho/Rheumatology Flashcards
What findings are present with a clubfoot?
What is the initial recommended treatment for this?
“CAVE”
- Cavus
- Adductus of forefoot
- Varus
- Equinus
Serial manipulation and casting using Ponseti method (<10% require surgery)
- Treatment should be initiated in all infants and should be started as soon as possible following birth
What is the diagnosis?
What kind of x-rays should you order?
List common radiographical findings for this presentation.
List 3 risk factors for this presentation

Slipped Capital Femoral Epiphysis (SCFE)
Radiographic findings:
- Widening of the joint space
- Femoral head is displaced posteriorly and inferiorly in relation to the femoral neck
Risk Factors
- Obesity
- Hypothyroidism
- GH deficiency
- Chronic renal failure 2˚ hyperparathyroidism
- Femoral retroversion
What is the diagnosis?
List common radiographical findings for this presentation.
What are 2 associations seen with this diagnosis?
What is generally the recommended treatment if slight restriction in ROM and minimal pain?

Legg-Calvé-Perthes disease
Radiographic findings
- Increased lucency of femoral head
- Widening of medial joint space compartment
- Flattened femoral epiphyseal ossification centre
ADHD, delayed bone age
Treatment
- Restricted activity
- ROM physical therapy
- Abduction bracing/casting
What is the diagnosis?
What screening examinations can be done for this diagnosis?
List 5 risk factors for this condition

Developmental Dysplasia of the Hip
Ortolani/Barlow <3 mo, then Galeazzi ≥3 mo (if bilateral, you lose the ability to compare the two)
Risk Factors
- Female
- First born
- Frank breech (really any breech in 3rd trimester)
- Family history
- Tight lower extremity swaddling
- Torticollis
- Foot abnormalities
- Large for gestational age
- Oligohydramnios
What are expected symptoms or signs associated with developmental dysplasia of the hip?
What are the screening recommendations for DDH?
What are indications for referral to orthopedic surgery?
How is DDH initially treated?
- Leg length discrepancy
- Asymmetric thigh or gluteal folds
- Limited or asymmetric abduction
- Abnormal gait (Trendelenberg)
- Positive Galeazzi sign (≥3mo)
- Positive Ortolani/Barlow (<3mo)
Screening
- Hip US between 6wks and 6mo for HIGH RISK with normal exam
- Hip XR (AP/frog pelvis views) >4mo
- Either test can be used between 4-6mo
Referral to orthopedic surgery
- Urgently: Unstable (positive Ortolani) or dislocated hip on clinical exam
- If positive Barlow, do US in 3-4 weeks then refer to Ortho if positive
- Limited hip abduction or asymmetric hip abduction after the neonatal period (4 weeks)
- Parental or pediatrician concern
Treatment
- Early(≤6mo): Pavlik harness
- Late (>6mo): Surgical intervention
List 2 possible diagnoses for a painless limp in a toddler.
List 2 additional diagnoses in a painless limp in a child (4-10yo).
Toddler
- Developmental dysplasia of the hip
- Congenital limb deficiencies
- Neuromuscular conditions
Child
- Developmental dysplasia of the hip
- Congenital limb deficiencies
- Neuromuscular conditions
- Leg length discrepancy
- Discoid meniscus
List 4 possible diagnoses for a painful limp in a toddler.
List 4 diagnoses for a painful limp in a child (4-10yo).
List 4 diagnoses for a painful limp in an adolescent (10-18yo)
Toddler
- Toddlers fracture
- Osteomyelitis
- Septic arthritis
- Transient synovitis
- Reactive arthritis
- Juvenile idiopathic arthritis
- Tumours
Child
- Septic arthritis
- Transient synovitis
- Legg-Calvé-Perthes
- Osteomyelitis
- Discitis
- Juvenile idopathic arthritis
- Trauma
- Tumour
- Overuse apophysitis
- Osteochondritis dissecans
Adolescent
- Tumour
- SCFE
- Juvenile idiopathic arthritis
- Osteomyelitis
- Septic arthritis
- Osteochondritis dissecans
- Discoid meniscus
- Overuse syndromes
List 3 bone lesions located in each of the following areas:
Metaphyseal
Epiphyseal
Diaphyseal
Metaphyseal
- Nonossifying fibroma
- Unicameral bone cyst
- Osteochondroma
- Osteomyelitis
- Osteosarcoma
Epiphyseal
- Chondroblastoma (most common)
- Eosinophilic granuloma
- Osteomyelitis
Diaphyseal
- Ewings sarcoma
- Eosinophilic granuloma
- Fibrous dysplasia
What is this lesion

Osteochondroma
- One of the most common benign bone tumours in children
- Many are completely asymptomatic
- Can have a genetic component (multiple hereditary exostoses)
- Usually in distal femur, proximal humerus or proximal tibia
- Enlarges with child until skeletal maturity
- XR: “stalks” or broad-based projections from the surface of the bone
- Complications: Foot drop
- Treatment is based on symptoms
What is this diagnosis?
Where is it most commonly located?
Where can it go?

Osteosarcoma - “sunburst appearance” - periosteal new bone formation
Metaphysis (Distal femur > Proximal tibia > humerus)
Lungs, bones
What is this diagnosis?
Where is it most commonly located?
Where can it go?
What is associated with poor prognosis?

Ewing’s sarcoma - “onion peel” appearance on XR
Diaphysis (lower extremity > pelvis > chest wall)
What is this diagnosis?
Where is it most commonly located?
How is it managed?

Osteoid osteoma
Most common benign bone tumour
Long bones in lower extremities
Observation (most resolve on their own)
If painful: NSAIDs, CT-guided radiofrequency ablation
What is this?
How does it present?

Sever’s disease (calcaneal apophysitis)
2˚ high impact sports - sharp lingering pain under the heel with activity and loading
What is this?
What is the name of a similar disorder with a different location?
How does it occur?
Give 3 treatment recommendations.

Osgood-Schlatter Syndrome (tibial tubercle)
Sinding-Larson-Johansson Syndrome (inferior patellar pole)
Overuse (repetitive strain) from jumping or kneeling
- Limit activities that exacerbate pain and reach pain-free state x 1-2 weeks before reintroduction and advancement
- Knee pads if chronic kneeling
- Self-directed stretching regimen, concentrating on quadriceps and hamstrings to address contributing factors (muscle tightness) during the rest period
- NSAIDs
What is this diagnosis
What are the exacerbating factors?
Where is the injury most commonly located?
What 2 ways would you treat this?
Spondylolysis
Repetitive spinal hyperextension (gymnasts, football interior linemen, weight lifters, wrestlers)
Most common at L5 - defect in pars interarticularis
- Restriction from exacerbating activities until pain free, then gradual reintroduction
- Physical therapy for core strengthening
What are 3 grades and their respective management.
List 4 indications for surgical referral.

- Mild (10 to <25˚): observation
- Moderate (25-45˚): bracing if growing; if growth completed, observation
- Severe (>45˚): spinal fusion considered (>50˚ thoracic, 40-45˚ lumbar and thoracolumbar)
Surgical Referral
- >45˚ Cobb angle
- Young age <11yo
- Double curves
- Failed medical intervention (bracing)
What are the Ottawa ankle rules for children?
What age can they be applied to?
- Must have pain in the malleolar zone AND ≥1 of:
- Tender along posterior aspect of lateral malleolus (distal 6cm)
- Tender along posterior aspect of medial malleolus (distal 6cm)
- Inability to bear weight IMMEDIATELY after injury AND in the emergency room
≥6 years old
What is the injury?
How is it caused?
How is it treated?
When should you consider XR?

Nursemaid’s elbow - Radial head subluxation
Traction on an extended and pronated forearm
Reduction = apply pressure to subluxed radial head while manually supinating the forearm and then maximally flexing the elbow
Consider XR if not using arm after maneuver
What 5 criteria do you look at to assess probability of a septic arthritis?
How high would you expect the WBC count to be on aspiration?
- ESR >40
- CRP >20
- Fever >38.5˚C
- WBC >12
- Inability to weight bear
>50,000 WBC with >75% PMNs
What is this diagnosis?
List 2 risk factors
What is the common radiograph finding

Tibia vara (Blount disease) - Infantile <3yo, Adolescent >10yo
Risk factors: obesity, early walking, Black or Hispanic ethnicity
XR: medial metaphyseal beak, internal tibial torsion, leg-length discrepancy
What are 2 complications associated with Pavlik harnesses?
List 2 ways to diminish these complications
Complications
- Avascular necrosis
- Temporary femoral nerve palsy
- Obturator (inferior) hip dislocation)
Diminish complications
- Stop treatment after 3 weeks if hip does not reduce
- Avoid forced abduction in the harness
- Ensure proper strap placement with weekly monitoring
Describe the expected course of lower extremity alignment (genu varum/valgum) with normal growth and development
Genu varum is at maximal point from 6-12 months
Neutral by 18-24 months
Maximum genu valgum is reached by 4yo (should not increase based 7yo)
What is the diagnostic criteria for SLE?
≥4/11. - “SOAP BRAIN MD”
- Serositis (pleuritis, pericarditis)
- Oral ulcers (or nasal; usually painless)
- Arthritis
- Photosensitivity
- Blood (hemolytic anemia or cytopenia [pancytopenia possible])
- Renal (nephritis; proteinuria >0.5g/day or cellular casts)
- ANA
- Immunologic (+ve ds-DNA or anti-Smith Ab or antiphospholipid antibodies)
- Neurologic (seizure or psychosis)
- Malar rash
- Discoid rash
What is the most sensitive test for lupus?
What is the most specific test for lupus?
What are other laboratory findings outside of the diagnostic criteria?
Sensitive: ANA
Specific: antu-Smith, anti-ds DNA
- Hypogammaglobulinemia
- Hypergammaglobulinemia
- False-positive RPR and VDRL tests
What are clinical symptoms of macrophage activation syndrome?
What are characteristic laboratory findings?
What is the management (3)?
- High-spiking fevers
- Lymphadenopathy
- Hepatosplenomegaly
- Encephalopathy
Labs (s-JIA MAS ↑ferritin + ≥2 of bolded):
- Thrombocytopenia
- Leukopenia
- Elevated liver enzymes, LDH, ferritin, triglycerides
- Prolonged coagulation testing: PTT/PT
- Low ESR
- Low fibrinogen
Treatment
- High-dose IV steroids
- Cyclosporine
- Anakinra
- Consider etoposide
What are the most common findings with HSP?
What is the management?
List 2 complications of HSP
IgA vasculitis
- Age >8yo
- Abdominal pain
- Recurrent palpable purpuric rash (can recur up to 4mo after initial presentation)
- Nondeforming arthritis/arthralgias (oligo-, large joints)
- Nephritis (Normal C3)
- Normal platelet count
- Mild anemia
- Elevated: Leukocytosis, thrombocytosis, ESR/CRP, IgA
Management
- Supportive
- Ensure adequate hydration, nutrition and analgesia
- Severe manifestations: corticosteroids, IVIG, plasmapheresis
- BP and UA monitoring for at least 6mo after diagnosis
Complications
- Intussusception
- Renal disease (can develop up to 6mo after diagnosis)
- Stroke
- Myocardial Infarction
- Mesenteric ischemia
What is the diagnostic criteria for systemic JIA?
Fever ≥2 weeks (daily “quotidian” for ≥3 days)
AND
Arthritis in ≥1 joint (follows fever)
AND ≥1 of:
Rash (evanescent)
Lymphadenopathy
Hepatomegaly or splenomegaly
Serositis
How long do you need to have symptoms to obtain a diagnosis?
List the different types of JIA + typical age presentation
Which is the only type of arthritis more common in males?
≥6 weeks
- Systemic (childhood)
- Enthesitis-related arthritis (late childhood/adolescence)
- Psoriatic (biphasic [2-4yo, 9-11yo])
- Oligoarthritis (1-4 joints during first 6mo) (early childhood 2-4y)
- Persistent (never >4 joints)
- Elevated (after first 6mo, more joints affected)
- Polyarthritis (≥5 joints during first 6mo)
- RF positive (≥2 occasions, ≥3mo apart) (late childhood/adolescence)
- RF negative (biphasic [2-4yo, 6-12yo])
- Undifferentiated
More common in males = Enthesitis-related arthritis
What is the diagnostic criteria for psoriatic arthritis?
Arthritis + Psoriasis
OR
Arthritis AND ≥2 of:
Dactylitis
Nail pitting
Family history of psoriasis in 1˚ relative
What is the diagnostic criteria for enthesitis-related psoriasis?
Arthritis or enthesitis AND ≥2:
SI tenderness or lumbosacral pain
Presence of HLA-B27 antigen
Onset in male >6yo
Acute anterior uveitis
FMHx 1˚ relative of HLA-B27 associated disease
What are the ophthomological screening recommendations for JIA?
Who is the highest risk?
-
High Risk (q3-4 months)
- Oligoarticular or polyarticular <7yo + ANA positive
-
Medium Risk (q6 months)
- Oligoarticular or polyarticular <7yo + ANA negative
- Onset >7yo regardless of ANA status
-
Low Risk (q1 year)
- Systemic JIA
Risk factors
- ANA positive
- Female
- Oligoarthritis
- Younger age
List 3 complications associated with JIA
- Iridocyclitis (chronic anterior uveitis) - can lead to permanent blindness
- Growth disturbances (leg length discrepancy)
- Micrognathia (TMJ arthritis)
- Osteopenia/osteoporosis
- Permanent joint damage requiring joint replacement
- Anxiety
When should a referral to orthopedics be considered for:
Metatarsus adductus
Tibial Torsion
Femoral anteversion
-
Metatarsus adductus:
- Persistent deformity and functional deficit
-
Tibial Torsion (>15˚ internal rotation):
- Persistence ≥7yo WITH deficit
-
Femoral Anteversion (>70˚ internal w/<20˚ external):
- Persistence ≥9yo WITH deficit
What are the clinical findings associated with Familial Mediterranean Fever?
What complication is associated with this periodic fever syndrome?
What is the recommended prophylaxis?
What is unique about the period in between their illnesses?
- Fever (brief) 1-3 days
- Painful Polyserositis
- Peritonitis
- Arthritis (mono-hip, knee, ankle)
- Pleuritis (unilateral) or pericarditis
- Erysipeloid rash (over ankle or dorsum of foot)
Complication: Amyloidosis → Renal Failure
Prophylaxis: Colchicine (decreases frequency, duration and intensity of flares + prevents development of systemic AA amyloidosis)
In between illnesses: infalmmatory markers remain elevated
What does PFAPA stand for?
When does it usually start?
How is it usually managed?
- Periodic Fever
- Aphthous ulcers
- Pharyngitis (exudative-appearing)
- Adenitis
<5yo; predictable recurrent fevers, lasting 4-6 days, occuring q3-6wks
During episodes: mild HSM, mild leukocytosis, elevated acute phase reactants
Management:
- Glucocorticoids (can increase frequency) - single PO dose (0.6-2mg/kg)
- Cimetidine (30% effective)
- Colchicine (30% effective) - may extend time between flares
- Tonsillectomy if medical management refractory
What is the diagnostic criteria for Juvenile dermatomyositis?
What is the recommended management?
- ≥2 of:
- Proximal symmetrical muscle weakness
- Elevated muscle enzymes (CK, AST, LDH or aldolase)
- EMG → myopathy and denervation
- Muscle biopsy → evidence of myositis (has largely been replaced with MRI showing proximal muscle inflammation)
Management
- High-dose glucocorticoids
- IVIG
- MTX for milder disease
- Hydroxychloroquine for cutaneous disease
What’s this finding?
What diagnosis is it associated with?

Gottron’s papules
Juvenile Dermatomyositis
What’s this finding?
What diagnosis is it associated with?

Heliotrope
Juvenile dermatomyositis
What’s this finding?
What diagnosis is it associated with?

Nail bed telangiectasias
Juvenile Dermatomyositis
List the diagnostic criteria for Kawasaki disease
List 3 supportive laboratory findings.
What is your management plan? Provide dosing.
What is the most common complication associated with this diagnosis? List 2 populations at increased risk for this.
- Fever ≥5 days AND ≥4:
- Bilateral non-exudative conjunctivitis
- Polymorphous rash
- Peripheral extremity changes (Plantar/palmar erythema or swelling, periungual desquamation)
- Changes in lips and oral cavity (oropharyngeal erythema, strawberry tongue, lip cracking or erythema)
- Cervical lymphadenopathy (>1.5cm, usually unilateral)
Labs: Elevated WBC w/left shift, Anemia, Thrombocytosis, Low albumin, elevated transaminases, sterile pyuria
Management:
- ASA high-dose 80-100mg/kg/day divided q6h until fever resolves, then 3-5mg/kg/day until inflammatory markers, platelet count and f/u echo are normal
- IVIG 2g/kg x 1 dose (monitor for hemolysis w/Hgb)
- Echocardiogram, repeated at 6-8 weeks following defervescence
Complication: Coronary artery lesions (dilatations, aneurysms)
Risk factors for coronary aneurysms:
- Male sex
- Extremes of age
- Prolonged fever
What is the difference between CRPS1 and CRPS2?
What are key features of these disorders?
What is the best treatment for these disorders?
- CRPS1 (formally reflex sympathetic dystrophy): no evidence of nerve injury
- CRPS2 follows a prior nerve injury
Key Features
- Pain disproportionate to inciting event
- Persisting allodynia (heighted pain response to normally non-noxious stimuli)
- Hyperalgesia (exaggerated pain reactivity to noxious stimuli)
- Swelling of distal extremities
- Indicators of autonomic dysfunction (cyanosis, mottling, hyperhidrosis)
Treatment
- Multistage approach:
- Aggressive physical therapy (initiated ASAP once diagnosis made) 3-4 times/wk
- May require analgesic prior to session
- Initially desensitization → weight-bearing, ROM→ functional activities
- CBT PRN
- Aggressive physical therapy (initiated ASAP once diagnosis made) 3-4 times/wk
- Pharmacologic
- Low-dose amitryptiline
- Sympathetic/epidural nerve blocks
What diagnosis is associated with:
Infant with a sudden onset of irritability, swelling of soft tissue and painful, wood-like induration with minimal warmth or redness and lack of suppuration overlying the mandible, clavicle or ulna.
Which bones are spared from this diagnosis?
List 2 complications.
What is the management?
Caffey disease (aka Infantile cortical hyperostosis)
Bones spared: phalanges, vertebral bodies
Complications
- Pseudoparalysis of limb
- Pleural effusions
- Torticollis
- Mandibular asymmetry
- Bone fusion
- Bone angulation deformities
Management: Indomethacin, corticosteroids (prednisone if indomethacin not effective)
When to treat Adolescent Idiopathic Scoliosis?
Treatment:
- Mild curves (<25 degrees) = Observation
- Moderate curves (25–45 degrees)
- If no growth remaining = Observation
- If still growing = spinal bracing to try to prevent/slow curve progression
- Severe deformity (>50 degrees) = spinal fusion surgery
You are seeing an 18 month old baby with a femur fracture. The baby has not had any previous long bone fractures, but there is a history of rib fractures in the past. You are concerned about non-accidental trauma, but feel that you should rule our Osteogenesis Imperfecta. a. Name 3 physical features that would support a diagnosis of OI.
Blue sclera Early deafness Easy bruising Joint laxity Short stature (ranges from mild to severe depending on type of OI) Bowing of long bones
Child presents with abdominal pain and arthritis. Picture of purpura on buttocks. A) What is the diagnosis? B) What is the MOST likely cause of long-term morbidity?
A) Henoch-Schonlein purpura B) Renal disease and hypertension (needs to be monitored for 1 year after episode)
Child with monoarticular JRA involving one knee. List 3 long-term orthopedic complications of arthritis.
- leg length discrepancy 2. flexion contractures 3. osteoporosis (from glucocorticoid use)
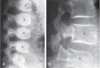
A 13 year old girl comes to you with a complaint of hip pain for the last month and a slight limp. You do the following hip XR. What is the diagnosis (shows dislocation of femoral head): a. SCFE b. AVN c. JIA
a. SCFE Classic presentation is limp with externally rotated, adducted leg - external rotation increases as hip is flexed
What is true in this child. Hip x-ray shown = SCFE a) sports-related trauma b) more frequent in females c) associated with steroid use d) subsequent bone necrosis
d) subsequent bone necrosis (AVN); other complication is chondrolysis (acute dissolution of articular cartilage in hip) ● Classic: obese, African American boy btwn 11-16 y.o. ● RF/ Trends o Black o Obesity o Male o Left > Right o Bilateral in 60% of cases
How do you classify a SCFE as stable vs unstable?
If they can walk on it, it is stable - but they should not walk on it because this can cause it to become unstable
28 week baby currently ventilated for severe RDS. Also has associated anomaly (picture of club foot). What to do: 1. Refer to ortho immediately for serial plastic (did not say plaster) casting 2. Refer to ortho once off ventilator 3. Refer to ortho at discharge 4. Refer to ortho at 3 months of age
- Refer to ortho at discharge - ideally casting should be started within the first month of life, but for prems in the NICU can defer treatment several weeks until foot has grown and infant has stabilized (do not start casting in NICU)
What are the components of a club foot and what is it’s medical name?
Talipes equinovarus Cavus - plantar flexion of first metarsal Adductus - of forefoot and midfoot Varus - hindfoot Equinus - hindfoot CAVE is also the order it is corrected in
Child with achondroplasia. Which is true: a. decreased life expectancy b. despite small foramen magnum, they rarely get cord compression c. borderline to mild developmental delay d. spinal stenosis commonly occurs in childhood
b. despite small foramen magnum, they rarely get cord compression - intelligence is normal unless CNS complications develop (e.g. hydrocephalus) - with appropriate intervention and monitoring risk of cord compression at foramen magnum can be minimized
Babe with clubfoot - name ONE part of the treatment.
Weekly casting using Ponsetti technique Most need tenotomy for equinus at end of casting Then bracing (boots and bars)
Which feature is typical for achondroplasia? a. proximal limb shortening b. distal limb shortening c. short mid-portion of the bone d. non-specific shortening
a. proximal limb shortening aka rhizomelic shortening of the arms and leg
A 12 year old boy comes to you with a complaint of left knee pain and swelling for the past month. He has also had pain over the right heel. Which of the following would you expect to find on family history: a. Psoriasis b. Ankylosing spondylitis c. Rheumatoid arthritis
b. Ankylosing spondylitis - enthesitis (inflammation at tendon insertion point) common - juvenile ankylosing spondylitis: - boys > girls - begins often with oligoarthritis and enthesitis - arthritis commonly in lower extremities and often hips
In an adolescent with pain below the knee after running, the x-ray shows changes compatible with Osgoode-Schlater’s disease. All are done except : a. Protective gear b. Ice may be used to reduce swelling a. Only stop activities which cause pain c. Quadriceps strengthening exercises when pain resolves d. Cast for 3-4 weeks
d. Cast for 3-4 weeks - mgmt: - rest and gradual reintroduction of activity (maintain activity level for 1-2 weeks before advancing) - if more severe, can use knee immobilizer or crutches until pain resolves - stretching quads and hamstrings while resting can help prevent recurrence once exercising again
Child with 6 wk history of severe ankle pain. Unable to weight bear. Unable to do physiotherapy. The foot is swollen, red, and warm. What is the most likely cause? a) Reflex sympathetic dystrophy (now called CRPS) b) Osteomyelitis c) Munchaussen
b) Osteomyelitis (no hx of fever, systemic unwell? BUT WARM joint is not CRPS and most likely osteo > CRPS epidemiology wise)
14 year old boy presents with groin discomfort. X-ray shown shows femoral neck and femoral head not aligned in the middle. What is your diagnosis (1)? What are two steps in management ? What are two risk factors for this disease (2)?
- SCFE 2. admit and put on bed rest - no weight bearing - consult ortho (who will pin in the OR) 3. RF: obesity, male, pubertal, endocrine disease (hypothyroid, hypopituitary, renal osteodystrophy)
What child with a SCFE would need further investigation for an underlying cause? What causes would you worry about?
Child under age 10 years - r/o endocrinopathy -hypothyroid, hypopituitarism, renal osteodystrophy)
What are risk factors for Legg-Calve-Perthes?
AKA AVN - trauma, family history, low birth weight
Description of a 4 yr old girl who refuses to weight bear. On exam, the only finding is there is tenderness over the proximal tibia (on both sides), What are your two differential diagnoses.
- leukemia 2. tibial stress fractures 3. toddler’s fracture (9months - 3 years, and distal tibia) 4. enthesitis/arthritis
Description of child with serum sickness day 10 of abx for URTI, joint pain, anemia, rash, hematuria. Management: a) Pulse pred b) IVIG c) high dose NSAIDS d) plasmapheresis
a) Pulse pred - appropriate for severe reaction - otherwise usually supportive management with NSAIDs (regular dose)
Picture of SCFE, how to treat: a. trial of NSAIDS b. “nail the hip” c. traction d. casting e. arthrocentesis
b. “nail the hip”
1 year old child presents with a metaphyseal femur fracture. What is the next step? a) calcium, phosphate and alkaline phosphatase levels b) full skeletal survey c) bone scan d) no further investigations
b) full skeletal survey CML’s= classic metaphyseal lesions= chip or corner #; bucket handle (high specificity for abuse) o Looks like chip off corner of long one o Thought to happen when pulled or swung violently and relatively weaker growing point of bones break - skeletal survey should be done in any child under 2 years with suspicion for abuse or under 5 years with suspicious fracture
A 6-month-old child has not been moving her left leg. An x-ray demonstrates a fracture at the corner of her distal tibia (metaphyseal bucket-handle fracture). What should be done: a) calcium, phosphate, and alkaline phosphatase levels b) screen for osteogenesis imperfecta c) skeletal survey d) bone scan e) no further investigations
c) skeletal survey
A 3 yo child develops left hip pain following URTI. What is the best way to rule out osteomyelitis? a) Lack of fever b) Normal WBC c) Negative blood culture d) Bone scan
d) Bone scan - WBC may be increased or normal - ESR and CRP are usually elevated - 50% of cases have positive blood culture - sensitivity of bone scan 90%, MRI more specific
A 2 yo boy is brought in by mom not moving left arm. He’s holding it pronated. Mom admits she pulled on Left wrist during horseplay. Pt not cooperative with exam. Next test: a) sling with xray b) sling then orthopedics referral c) orthopedics referral d) skeletal survey e) manipulate at elbow until arm function restored
e) manipulate at elbow until arm function restored - rotate arm into supination while maintaining pressure over radial head until click is felt
Xray of a child/infant’s elbow…story goes that it is painful, but there is no swelling and the parents brought the child in (I think he was 10 months old?) no hx of trauma. No fever. What is your diagnosis? What could have caused this?
Pulled elbow (subluxation of radial head with annular ligament slipping between radial head and distal humerus). Caused by longitudinal traction force applied at elbow (e.g. someone pulling on child’s arm to stop them from falling) - full flexion and extension but limited supination
Dad brings toddler to ED for shoulder pain, xray shows spiral fracture. List the next three things you do.
Assuming there is no clear mechanism of injury… 1. skeletal survey 2. contact child protective services 3. immobilize fracture, consider advice from ortho if needed 4. pain control
9 month old boy who has come in with a story of an accident. Nurse mentions he has been in her 5 times previously with other injuries. He is a well child otherwise.. Picture of Xray of bones with bony chip off the distal humerus. (1) What does the xray show (2) What could have caused this
- classic metaphysical lesion of distal humerus 2. physical abuse - accidental trauma - this type of fracture is caused by accumulation of multiple micro fractures across the metaphysics perpendicular to the axis of the long bone (from shaking/shearing forces)
What is the most common childhood wrist fracture a. Colles fracture b. Greenstick c. Buckle fracture d. Salter Harris
b. Greenstick c. Buckle fracture - unclear which is correct ● 80% of forearm fractures involve the distal radius and ulna ● majority of forearm fractures are buckle or greenstick fractures - buckle (or torus): compression fracture - greenstick: bone bends, but only breaks on the convex side, not all the way through
You are seeing an 8 month old female with a femur fracture and are concerned about non-accidental trauma: a. What are the next 3 investigations that you will do to support your diagnosis?
- skeletal survey 2. liver enzymes (screen for abdominal trauma) 3. 25-OH-vitamin D, serum calcium, phosphorus, alkaline phosphatase (may be elevated with healing fractures), parathyroid hormone 4. U/A (for hematuria)
Young girl who has flat feet. Mum is concerned. When she stands the feet are flat and you note that they are valgus and that her forefoot is abducted. When she sits down with her feet in the air, her arches look normal. What is her diagnosis (1) ? What kind of intervention is needed for her (1)?
- Dx: hypermobile flexible pes planus 2. generally no treatment needed - common in young children and they generally outgrow it - if pain, abnormal wearing down of shoes, or fatigue after walking can consider treatment with orthotics (will help symptoms but not correct pes planus)
Child presents to ER with fever, sore hip what do you do? a. aspirate joint b. Xray hip c. order CBC
a. aspirate joint (concern for septic arthritis) dx: blood culture - aspiration of joint for gram stain and culture - WBC, CRP and ESR generally elevated but non specific and normal tests do not rule out septic arthritis - imaging - X-ray at least - surgical emergency
14 year old being treated for osteomyelitis. Severe pain despite naproxen and tylenol. Best analgesic: a. narcotic b. tricyclic c. higher dose of NSAID
a. narcotic - follow pain ladder - if giving regular tylenol and NSAID and not achieving good control then escalate to narcotic
A 14-year-old girl with spina bifida at the T12 level presents with a one-day history of a swollen leg and foot with erythema over the anterior tibia. Temp 37.8. WBC 16. ESR 22. Most likely:** a) fracture b) cellulitis c) osteomyelitis d) deep venous thrombosis e) erythema nodosum
b) cellulitis - sounds most like cellulitis - may have decreased sensation so less aware of developing infection - other thought was DVT as may be immobilized from spina bifida
18 mo M high fever, irritable, not moving hip. Next management issue? a. IV ABx and blood culture b. Needle aspiration c. X-ray
b. Needle aspiration
What is the position of the septic hip in a patient with septic arthritis? a) Abducted and internally rotated b) Abducted and externally rotated c) Adducted and internally rotated d) Adducted and externally rotated
b) Abducted and externally rotated
You are seeing a 19 month old boy who has a swollen right knee. A joint aspirate is positive on C&S for S. Aureus. He also has a history of a pneumococcal meningitis at 9 months of age. You order a CBCd, blood C&S and CT scan of the knee, and start him on IV antibiotics. a. What 4 further tests will you order?
Concern for immunodeficiency: - recurrent bacterial infections - think B cell, phagocytic and complement defects 1. immunoglobulins (IgG, IgM, IgA, IgE) 2. C3, C4, CH50 3. vaccine titres for antibody responsiveness 4. next line - lymphocyte phenotyping, antineutrophil antibody, sweat chloride, bone marrow biopsy 5. MRI to rule out adjacent osteomyelitis
Child with hip pain for 3 days. Today fever to 39, significant increase in pain. He is sitting with leg flexed and ext rotated. What are the 2 most important diseases on your differential diagnosis. List 3 investigations you would do to differentiate.
- septic arthritis of hip - osteomyelitis 2. MRI of hip - joint aspirate - U/S (for effusion and fluid collection)
Child presents with 6 week history of pain after mild ankle injury – now won’t bear weight, hurt to touch, hot, no objective signs of arthritis. What is the diagnosis? Treatment?
Dx: osteomyelitis Tx: IV antibiotics - depends on age but cefazolin a general good choice - tx duration 3-4 weeks - depends on clinical response
5 year old fever 38.5 degrees, had a recent URTI. Hip was externally rotated and child not weight bearing. ESR was 40. Diagnosis? a) Transient synovitis b) JIA c) Septic arthritis
c) Septic arthritis Kocher Criteria For septic arthritis ● T >38.5 ● WBC >12 ● ESR >40 ● Inability to weight bear ● CRP >23
A 2 y/o child with in-toeing. Father reports having had the same problem as a child for which he was fitted with immobilization boots. On exam, child has a searching toe, metatarsus adductus, and internal tibial torsion. What to do: 1. Observe 2. Discourage W sitting 3. Cast 4. Refer to ortho
- Observe *note: internal tibial torsion doesn’t need anything done but the metatarsus adductus should at least be treated with stretching (though most resolve spontaneously), and potentially casting depending on if it’s flexible or not. W sitting is related to internal femoral torsion, but you could still discourage it to prevent that from happening later - internal tib torsion: starts to correct as child begins walking - may correct as early as 4 years or up to 10 years
Parents bring 3 year old for intoeing gait. You find tibial torsion and flexible metatarsus adductus. His father had a similar condition. Neurologic examination is normal. You advise: a. stop W sitting b. ortho referral for in shoe prosthesis c. no treatment necessary as this invariably resolves d. Dennis splint e. x-ray of lower limbs
c. no treatment necessary as this invariably resolves Make sure metatarsus adductus is flexible and recommend stretching exercises
2-year-old child with flexible flat feet. Father and aunt had the same abnormality. You suggest: a) no intervention is necessary b) must wear shoes all the time c) needs orthotics d) foot exercises e) orthopedics referral
a) no intervention is necessary
An 18 month old infant of African immigrant parents presents to you because he is not cruising or walking. He was exclusively breastfed until the age of 6 months, and now eats mainly purees, fruits and vegetables. On examination there is prominence at his distal radius and ulna and medially at his proximal tibia. Which of the following lab abnormalities will support your diagnosis: a. Low PTH b. High ionized Ca c. Low 25-OH vit D d. Low ALP
c. Low 25-OH vit D Expecting Low Ca and Vitamin D in diet ● PTH high ● High Alk Phos (compensation) Rickets
An 8 year old boy with an unremarkable past medical history comes to you because his mother notices that he walks on his toes. a. Name 4 causes of bilateral toe walking.
- should walk heel-toe by age 4 - refer to ortho if still toe walking by 4 - Causes o Idiopathic (no abnormalities on exam, just when walking), +/- Heel cord contracture o Cerebral Palsy o Duschenne Muscular Dystrophy o Tethered spinal cord o Autism spectrum disorder
Best determinant of scoliosis on Physical Exam. 1. leg length discrepancy 2. asymmetric shoulder height 3. asymmetric ribcage on bending over 4. asymmetry on lateral flexion
- asymmetric ribcage on bending over
14 yo girl with idiopathic scoliosis. Give 3 indications for referral to ortho.
Ix: standing PA and lateral of entire spine and calculate Cobb angle Referral: - progression of curve by 5-10 degrees - curve >20 degrees (prepubertal) or >30 degrees (pubertal) - left curve - pain - abnormal PFTs
14 yr old who hasn’t been to see you in 2 yrs. She has scoliosis with Cobb angle of 50 degrees. What is the most appropriate management? a. observe b. refer for brace/ orthosis c. refer for posterior spinal fusion d. electrical muscle stimulation
c. refer for posterior spinal fusion - likely postmenarchal and has high degree curve - bracing unlikely to be effective
Teen post op scoliosis repair. Day 6. Billious vomiting. Weight loss. ABdo pain. What is most likely complication? a) Superior mesenteric artery syndrome b) Adhesions c) Volvulus
a) Superior mesenteric artery syndrome
3 yo girl generally well but has had 3 weeks of right knee swelling. Best initial treatment? a. Steroids b. Methotrexate c. NSAIDS
c. NSAIDS - tx for transient synovitis: NSAIDs and limitation of activity - can take up to 2 weeks for resolution of symptoms - ddx to consider: - septic arthritis - reactive arthritis (following enteropathic or urogenital infection) - post-infectious arthritis (following some other infection like viral URTI) - acute rheumatic fever - lyme arthritis - JIA
3 y/o with mono arthritis for a few weeks. What is the most likely test result: 1. Positive RF 2. Positive ANA 3. Increased WBC 4. Increased ESR 5. Decreased Hgb
- Increased ESR - most likely transient synovitis which can have mild increased in ESR and CRP
12 yo girl with arthritis, some blood in the urine. Three things on differential?
SLE HSP Post strep GN Systemic vasculitis
Child recovered from recent reactive arthritis. Has residual 30 degree painless flexion contracture of knee. Name 3 non-pharmacologic treatment modalities.
- stretching/physio - bracing - surgery - botox
Child with monoarthritis. Name 3 medications from different classes of medications that are used for treatment.
- NSAIDs: ibuprofen 2. Corticosteroids: prednisone 3. DMARDs: methotrexate 4. Biologics: infliximab 5. Immunosuppressants: cyclophosphamide
Boy had recent illness - fever, diarrhea, conjunctivitis, urethritis now with sacroilitis. You diagnose him with Reiter syndrome. List 4 organisms that could cause Reiter syndrome.
Reiter syndrome: reactive arthritis with uveitis and urethritis - following GI or GU infection - “can’t see, can’t pee, can’t climb a tree” - salmonella - shigella - yersinia - campylobacter - chlamydia Post infectious arthritis - not GU/GI specific - strep, Hep B, rubella, parvo B19, varicella, CMV
Which of the following is the best confirmatory test for juvenile dermatomyositis? a. EMG b. CK c. ANA
a. EMG - key features are proximal muscle weakness and heliotrope rash and Gottron’s papules
What are the diagnostic criteria for juvenile dermatomyositis?
heliotrope rash/Gottron’s papules + 3 of: - symmetric proximal muscle weakness - elevated of 1+ muscle enzymes (CK, AST, LDH) - EMG changes - muscle biopsy showing inflammation (only indicated if diagnosis is uncertain or to grade severity)
12 year female with a 2 week history of fever, polyarthralgia. Looks well, but pale. T=37.6. No joint swelling. Trace protein and blood in urine. Normal creatinine. Most likely diagnosis is: a. systemic JIA b. SLE c. rheumatic fever d. Goodpasture’s syndrome
b. SLE - most common complaints in kids are fever, fatigue, hematologic abnormalities, arthralgias and arthritis (symmetric polyarthritis) - renal involvement usually asymptomatic so need to look for it (HTN, proteinuria, hematuria, edema, nephrotic syndrome, renal failure) Note: *arthritis must be present to diagnose ANY type of JIA - Goodpasture: pulmonary hemorrhage and glomerulonephritis
What is the diagnostic criteria for JIA? How do you classify it?
- arthritis (dx of arthritis = swelling OR 2 of decreased ROM, pain with motion, warmth) - duration 6 weeks minimum - classify based poly (5+ joints involved in first 6 months after onset), oligo (1-4 joints), or systemic onset (arthritis with fever and rash)
10-year-old girl with a 1 week history of fever (not greater than 38.5) and migratory arthritis. On examination there is evidence of arthritis in the right wrist, but the rest of the exam is normal. WBC is 25 with a left shift. ESR 45. Most likely diagnosis: a) acute rheumatic fever b) juvenile rheumatoid arthritis c) systemic lupus
a) acute rheumatic fever Jones criteria - 2 major OR 1 major and 2 minor Minor: elevated ESR, CRP, temp 38.5, arthralgia
Child presents with fever, polyarthritis, increased ESR and ASOT=625. Echo is normal. Best management:
Mgmt of acute rheumatic fever without heart disease: 1. ASA for fixed period (dosing progressively lowered over 6 weeks, then stopped) 2. Pen V for 10 days to eradicate strep infection 3. Strep prophylaxis: Pen G benzathine IM q4 weeks, or BID Pen V or daily sulfasalazine until age 21
Child with a 2 week history of migratory arthritis, fever 38.5, a normal echo, WBC 18, ESR 75, throat swab negative, and an ASOT > 625. What should you do: a. ASA 100mg/kg until arthritis resolves b. ASA prn pain, treat 10 days with penicillin c. ASA 100mg/kg until arthritis resolves, treat 10 days with penicillin d. ASA 100 mg/kg until arthritis resolves, treat 10 days with penicillin followed by q monthly IM penicillin e. ASA 100mg/kg until arthritis resolves, treat 10 days with penicillin, oral penicillin for dental procedures
d. ASA 100 mg/kg until arthritis resolves, treat 10 days with penicillin followed by q monthly IM penicillin
8y female with subtle choreoathetotic movements. Handwriting has worsened and she is emotionally labile . Evaluations including a throat culture are negative. What is the most likely diagnosis? a. Huntington’s chorea b. Syndenham’s chorea c. SLE
b. Syndenham’s chorea - chorea, emotional lability and hypotonia/incoordination and pronation of the hand causing difficulties writing are all classic features - culture and ASOT often negative as can occur months after strep infection - treat with long term antibiotic prophylaxis - chorea resolves in 6-9 months
Rheumatic fever – which most likely causes long-lasting problems? a) carditis b) chorea c) nodules d) Polyarthritis
a) carditis - cardiac is long-term sequelae of ARF
Child has a history of recurrent fevers, evanescent pink rash, lymphadenopathy, hepatomegaly. His musculoskeletal exam is normal. What’s the diagnosis? a) Leukemia b) Scarlet fever c) Lyme disease d) Systemic JIA
d) Systemic JIA - fevers once-twice daily for at least 2 weeks, and unwell during this time Dx: arthritis in min. 1 joint x2 wks with, or preceded by, fever documented daily (“quotidian”) x 2 weeks and accompanied by min 1 of o Evanescent (nonfixed) erythematous rash (macular, non pruritic, transient +/- crops over trunk + limbs) o Generalized lymph node enlargement o Hepatomegaly or splenomegaly or both o Serositis
What are some prognostic factors for systemic onset JIA?
Systemic JIA worse prognosis in general - worse prognosis if: - polyarticular - fever >3 months - increased inflammatory markers on BW x>6 months
Features of Kawasaki disease include all EXCEPT: a) elevated WBC (yes) b) ANA negative (yes) c) platelet count 75 d) urine with 10-15 WBC/hpf (yes)
c) platelet count 75 ● Leukocytosis, Anemia, Thrombocytosis after week 1 ● Elevated CRP and ESR ● Hypoalbuminemia ● Hyponatremia ● Abnormal plasma lipids ● Sterile pyuria ● Elevated serum transaminases and GGT ● Pleocytosis of CSF ● Leukocytosis in synovial fluid
Kawasaki dz, parents refuse IVIG. What is an acceptable alternative? a) ASA b) ASA + steroids c) ASA + cyclophosmide d) steroids alone
b) ASA + steroids - ASA always anyway - steroids second line
3 year old with a history of fevers. Occur every 4 to 12 weeks for 1-4 days. Growing well. Treated for numerous otitis and pharyngitis. A) multiple viral infections B) familial med fever C) CVID
A) multiple viral infections
List 5 warning signs of primary immunodeficiency
- 4 new ear infections in a year 2. 2 serious sinus infections in a year 3. 2 pneumonias within a year 4. 2 deep seeded infections in life 5. 2 months on antibiotics with little effect 6. needing IV abx to clear infection 7. recurrent abscesses 8. persistent thrush or fungal infection 9. FTT 10. family hx of primary immunodeficiency
A 12-year old female presents with a two-week history of fevers, arthralgias, and myalgias. She is pale but otherwise looks well. She has blood and protein in her urine. WBC 18. Platelets normal. a) acute rheumatic fever b) Wegener’s granulomatosis c) systemic lupus erythematosus d) juvenile rheumatoid arthritis
c) systemic lupus erythematosus - arthritis, anemia, arthralgia, renal disease in a 12 yo female - fits with SLE - classic presentation SLE: fever, rash, renal, MSK, heme (anemia, leukopenia, TCP) - Wegener’s: granulomatosis with polyangiitis: respiratory symptoms (SOB, cough), fatigue, malaise, fever and renal involvement so is possible BUT less common
What is the diagnostic criteria for SLE?
4/11 of SOAP BRAIN MD - at least 1 clinical and 1 immunologic - serositis (pleuritis, pericarditis) - oral or nasal ulcers - arthritis (oligo or poly) - photosensitivity - blood cells (all lines low) - renal (nephrotic) - ANA+ - immune markers + (anti-Smith, anti-dsDNA, anti-phospholipid) - neuropsych (seizures, psychosis) - malar rash - discoid rash
(Picture of a child with an erythematous rash over the face, concentrated over the upper eyelids, and over the MCPs and PIPs) A 6 year old boy comes to you with a history of progressive fatigue over the past month. You note the following rash on physical examination. a. What is your diagnosis? b. Name 3 tests that will help to confirm your diagnosis. c. What one medication would you consider starting at this point?
a. juvenile dermatomyositis b. muscle enzymes (CK, AST, LDH) - EMG - muscle biopsy - proximal muscle weakness - positive Gower’s c. steroids (mainstay of treatment)
Boy with Kawasaki’s disease. Give 5 criteria for Kawasaki’s
5 days of fever - cervical LAD >1.5cm - bilateral non-purulent conjunctivitis - swelling/redness/peeling of hands and feet - rash (diffuse, maculopapular) - oral membrane involvement (cracked, red lips, strawberry tongue, pharyngitis)
14 year old boy with low back pain. You suspect ankylosing spondylitis. What are 2 findings on physical exam? What are two tests to help you in this diagnosis? How is this treated?
- SI tenderness on FABER test - Schober test (15cm span marked starting at level of iliac crest while standing) - distance measured after forward bend - positive if distance increases by <5cm 2. ESR and RF normal - HLA B27 positive - XR: late findings identified like squaring of vertebral bodies - MRI: bone marrow deem adjacent to joint 3. NSAIDs, intra-articular steroids, DMARDs, physio
Neonate with thrombocytopenia, elevated liver enzymes, target lesion rash. What is the diagnosis?
Neonatal lupus
Kid with JIA, high fever, hypotensive, high ferritin and high trigs, pancytopenic. what is the ddx:
macrophage activation syndrome - occurs most often in first weeks to months after onset of JIA symptoms, though can happen any time in course of disease Diagnostic criteria - 3/5 of: - fever >38.5 - splenomegaly - cytopenia (at least 2/3 cell lines) - increased triglycerides OR low fibrinogen - elevated ferritin (often >1000, must be >500)
(Picture of a kid with a malar rash). Has fever, joint pain, diffuse rash. Only meds are fluticasone and phenytoin for a seizure disorder. What is the most likely? a. drug hypersensitivity reaction b. Juvenile dermatomyositis c. Systemic lupus erythematosus d. Juvenile idiopathic arthritis
This could be drug induced lupus from phenytoin - drug induced lupus can be true SLE in a predisposed individual that is triggered by drug (this will not resolve) - or it can be a lupus-like syndrome that is caused by the drug and resolves after the drug is discontinued (though can take months to years for full recovery)
Rash over backs of hands, muscle pain, being teased at school for weakness. a. DMD b. JDM c. SLE
b. JDM
Evanescent rash, lymphadenopathy, hepatomegaly. What does this suggest? a. lupus b. systemic onset JIA c. kawasaki d. rheumatic fever
b. systemic onset JIA
A 7 year old boy has a history of recurrent fevers, evanescent pink rash, lymphadenopathy, and hepatomegaly. His MSK exam is normal. What’s the diagnosis? a) Leukemia b) Scarlet fever c) Lyme disease d) Systemic JIA
d) Systemic JIA *fits best with JIA, but very abnormal that the MSK exam is normal
4 yr old boy with fever of 40 degrees despite amoxcil. Maculopapular rash, bilateral conjunctivitis,dry cracked lips. What is the most likely lab finding? a. hypoalbuminemia b. neutropenia c. EBV monospot + d. + ASOT
a. hypoalbuminemia
Kid with >=6 day of fever, non purulent conjuctiviits, MP rash. Clinical picture c/w Kawaski’s dx. Most likely lab abnormality? a. Low albumin b. Neutropenia c. Monospot + d. Positive ASOT
a. Low albumin
Child with pulmonary findings, eosinophilia, slightly elevated calcium (2.8) a. miliary TB b. sarcoidosis c. cryptococcus d. blastomycosis
b. sarcoidosis - multisystem granulomatous disease of unknown etiology - older kids are like adults (mild pulmonary involvement - dry persistent cough, LAD) - early onset sarcoid (<4 years): rash, uveitis and arthritis - also nonspecific sx like fever, wt loss, malaise - CXR: bilateral hilar adenopathy - small percentage have hypercalcemia/hypercalciuria - leukopenia, TCP and eosinophilia can be seen
14 yr old with fevers, polyarthralgia, wt loss. Appears pale. No arthritis on exam. Urine + for protein and blood. Decreased WBC and lymphs. Normal platelets. What is the most likely diagnosis. a. SLE b. Systemic JIA
a. SLE
Child with wt loss anemia, normal plts, low WBC, protein/blood in urine. Dx? a. SLE b. RF c. PSGN
a. SLE ● most common presenting complaints of children with SLE include fever, fatigue, hematologic abnormalities, arthralgia, and arthritis → arthritis does not have to be present in a dx of SLE but definitely needs to be present in all forms of JIA
4 year girl with arthritis of two months duration. On exam she has a swollen elbow and knee. Her ANA is positive. What is her diagnosis?. What is one complication that she is at risk for. What would your initial treatment be (1) ?
- oligoarticular JIA 2. complication: chronic uveitis (girls with oligoarthritis who are ANA positive are highest risk of this) - can lead to cataracts and blindness 3. NSAIDs
Three ways that maternal SLE can affect neonate.
- heart block - thrombocytopenia - rash - hepatitis
14 yo girl with leg pain, which is worse after activity and at night. On examination there is tenderness and swelling above the knee joint but no effusion. A radiograph shows a lesion in the distal femur with periosteal elevation. What is the likely cause? a. osteoid osteoma b. osteogenic sarcoma c. subperiosteal hematoma d. osteomyelitis
b. osteogenic sarcoma - the description of periosteal elevation (aka onion skinning) is more typical for Ewing sarcoma, but these tumours are more common in kids under age 10 - osteomyelitis also possible, but pain worse at night suspicious for cancer
Pt with HSP. What would you do to monitor: a. urinalysis b. IgA c. Stool for o/b d. AXR
a. urinalysis Renal: weekly UA + BP while active clinical disease then monthly x 6 month (to R/O late onset renal disease) o If all (-) in this FU period then unlikely to develop nephritis after 6 months o If (+), HTN, renal failure, hematuria -> talk to nephro
Child with a head that looked like this - picture of infant with dolichocephaly. What is the diagnosis? What finding on physical examination would support this?
- craniosynostosis 2. closure of sagittal suture with no mobility, prominent boney ridge
Teen (gymnast) insidious onset lower back pain. Pain on extension, hamstring tightness. Paraspinal muscle spasm. Normal neuro exam. Positive TC99 scan. What is the dx. a) Spondyloarthropathy b) Spondylolysis c) Posterior element overuse d) Vertebral avulsion fracture
b) Spondylolysis spondylolysis ● anatomic defect (radiolucent gap) in pars interarticularis with adjacent bone sclerosis - develop over time, not present at birth ● mechanism → usually activity related and occurs from repetitive hyperextension - prevalence as high as 47% in certain athletes (gymnasts, weightlifters, football linemen) - can be seen on bone scan
Emotional lability and choreiform movements a. Tourettes b. SLE c. Huntingtons d. Sydenhams
d. Sydenhams
What is associated with higher risk of uveitis in JIA? What is the presentation?
- Oligoarthritis
- ANA positive
Usually asymptomatic, but can have synechiae (abnormal pupil shape), glaucoma, cataracts, vision loss
- Except in enthesitis related, its usually symptomatic (ie acute uveitis)
What are pain amplification syndromes?
- Generalized vs localized
- Generalized = fibromyalgia, specific trigger points, assoc psych Sx
- Localized = reflex sympathetic dystrophy, complex regional pain syndrome
- Can have autonomic changes (acute = swelling; chronic = atrophy/cold extremities)
- F > M
- Treatment: multidisciplinary assessment and therapy
Complex Regional Pain Syndrome (CRPS)
- No nerve injury, pain disproportionate to the inciting event, persistent allodynia, hyperalgesia, swelling and autonomic dysfunction (cyanosis, mottling, hyperhidrosis)
- Tx: 3P’s = Physio, psych, pharmacological
What labs are deranged in HLH/MAS?
- Cytopenias (usually plt and WBC)
- Decreasing ESR (from fibrinogen consumption)
- Decreased fibrinogen
- Increased ferritin
- Increased triglycerides
- Increased LDH and LFTs
- Prolonged PTT and INR
- Increased D-dimer
