Lecture Exam 2 Flashcards
What are the main functions of the respiratory system?
Gas exchange
Vocalization
Olfaction
Acid-base balance
ACE conversion / BP
Pressure Gradient establishment
Name the structures/pathway in order from the mouth/nose to the lungs
nose, pharynx, larynx, trachea, bronchi, bronchioles, alveoli

What does the conducting division of the respiratory system consist of?
(Structure and function)
Those passages that serve only for airflow, essentially from the nostrils through the major bronchioles
-
Upper respiratory tract
- Structure:
- Mouth, pharynx, epiglottis
- Function:
- Airflow
- Warm, cleanse, and humidify air
- Olfaction
- Structure:
-
Lower respiratory tract
- Structure:
- Glottis, larynx, trachea, bronchi
- Function:
- Airflow and cleansing
- “Mucous elevator”
- Vocalization
- Structure:
What are the respiratory division structures consist of and what are their functions?
-
Bronchioles
- smooth muscle
-
Alveoli
- Site of gas exchange
- Cellular specialization
- Squamous (Type 1) Cells = ~95% of cell
- Diffusion
- Great (Type 2) cells = ~5% of cell
- Repair and surfactant production
- Wandering macrophages
- Squamous (Type 1) Cells = ~95% of cell
- Respiratory membrane
- Squamous (Type 1) cell
- Basement membrane
- Capillary endothelial cell

Explain the details of the respiratory membrane
Include:
- Squamous alveolar cell
- Shared basement membrane
- Capillary endothelial cell

What are the inspiratory and expiratory muscles?
Inspiratory muscles:
- Diaphragm
- External intercostals
Expiratory muscles:
- Internal intercostals
- Abdominal muscles
Name and describe the neural control centers for the respiratory control and what they impact
Control of skeletal muscles
-
Medulla
- Ventral Respiratory Group (VRG)
- Active in bursts during quiet breathing
- Control activity of phrenic and intercostal nerve
- primary generator of respiratory rhythm
- Ventral Respiratory Group (VRG)
-
Dorsal Respiratory Group (DRG)
- Receives sensory input
- Modifies activity of the VRG
- Breathing is adapted to varying conditions
-
PONS
- Pontine respiratory group (PRG)
- Modifies activity of VRG and DRG
- Receives input from high brain centers
- eg. hypothalamus, limbic system, and cerebral cortex
- Adapts to sleeping, exercise, vocalization and emotional response changes
- Pontine respiratory group (PRG)
- Neural Output

Explain the types of stimuli and sensors (Who controls the control centers?)
-
Central Chemoreceptors
- Medulla oblongata - brainstem neurons
- respond to changes in pH of cerebrospinal fluid
- “Stimulating” stimuli:
- Increase CO2 (hypercapnia) or decrease pH of CSF
- Medulla oblongata - brainstem neurons
-
Peripheral Chemoreceptors
- Carotid and aortic bodies
- respond to O2 and CO2 content of the blood and pH
- Stimulating stimuli:
- Decrease PO2, Increase CO2, or Decrease pH in blood
- Carotid and aortic bodies
-
Stretch Receptors
- Found in smooth muscle of the bronchi and bronchioles and in the visceral pleura
- Respond to inflation of lungs and signal the DrG by way of vagus nerves
- Hering-Breuer reflexes (excessive inflation triggers this reflex)
- Inflation reflex
- Deflation reflex
- Prevent damage due to overexpansion or collapse
- Found in smooth muscle of the bronchi and bronchioles and in the visceral pleura
-
Irritant Receptors
- Detection of irritating chemicals / gases
- Trachea receptors trigger coughing
- Nose and pharynx receptors trigger sneezing
- Detection of irritating chemicals / gases
-
Voluntary Control
- Required for vocalization and swimming
- Neural bypass of respiratory centers under control of cerebral cortex

What is the fluid flow directly proportional to?
F = delta P / R
Where:
F = flow
Delta P = change in pressure
R = resistance
What is the pressure that drives respiration, explain
atmospheric (barometric) pressure
the weight of the air above us
Explain Boyle’s law
at constant temperature, the pressure of a given quantity of gas is inversely proportional to its volume
P1V1 = P2V2
Explain how the pressure difference in the lungs and chest cavity are impacted during the respiration cycle

Explain the breathing mechanistic gas physics, ie. ideal gas law
PV = nRT
(Boyle’s law)
P = pressure
V = volume
n = # of gas molecules
R = gas constant
T = temperature
Pressure and volume are inversely proportional
Air moves from high to low pressure
Explain the respiratory pressure changes during the respiration cycle
-
Atmospheric Pressure
- Air pushing down
- 760 mm Hg (at sea level)
- Since it doesn’t change, set to zero
-
Intrapulmonary Pressure
- Internal pressure in the lungs (in alveoli)
- Changes due to lung volume
- Normally -1 to +1 (relative to Patm)
- -1 = greater volume in lung
- +1 = lower volume in lung
- Normally -1 to +1 (relative to Patm)
-
Respiratory Cycle
- Inspiration
- Increase in lung volume = decreased intrapulmonary pressure
- Air flows in
- Inspiration
-
Intrapleural pressure
- Pressure in pleural space
- A ‘sucking’ force!
- Based on elastic pull inwards vs. adhesion outwards
- Varies during respiratory cycle
What are the factors that enhance pressure in the lungs?
Volume changes, most substantial effect
Adhesion of lung to pleural wall
Elasticity of the lungs and chest wall
Explain the factors enhancing resistance in the lungs
-
Airway diameter
-
Bronchoconstriction
- Histamine, PSNS
- for people with allergic response, this is how it is treated
- Histamine, PSNS
-
Bronchodialation
- Epinephrine, SNS
- beta 2 agonists
- in puffers for people with asthma
-
Bronchoconstriction
-
Pulmonary compliance
- Surfactant decreases surface tension
- very easy to fill up under normal circumstances, but as you get older the elasticity decreases
- Prevents collapse
- amphiphilic molecules that disrupts and prevents collapse
- Surfactant decreases surface tension
Explain alveolar ventilation, like breaths per minute for a normal adult and for a child
Adult normal = 12 / min
Children = 18 - 20 / min
Explain how to calculate the respiratory minute volume (VE)
Respiratory minute volume (VE) = F x Vt
where: F = breaths per minute, Vt = title volume
Normally 12 breaths/min x 500 ml/breath = 6 L/min
Variable by delta F or delta Vt
Up to 200 L/min
If your VE = 6.0 L/min, how many breaths per minute are you taking?
- cannot answer because you do not have the title volume (Vt)
Explain the alveolar ventilation (VA) and how to calculate it
Volume of ‘fresh’ air getting to alveoli
-
Automic dead space (VD)
- Air ‘left’ in conducting zone
- Only one way in and out, so the air mixes and that wish why you must subtract out the dead space when calculating the alveolarventilation
- ~150 ml per breath
- Air ‘left’ in conducting zone
-
VA = f ( Vt - Vd)
- VA = alveolar ventilation
- Vt = title volume
- VD = Automic dead space
- ex: VA = 12 bpm x (500 ml - 150 ml) = 4.2 L/min
- only about 2/3 of the air we breath is fresh
What are the anatomical dead space implications?
- If VE stays constant (6.0 L/min), but F goes down, what happens to VA
- how many breaths before VA = 0 L/min when VE = 6.0 L/min
- If F goes up and VE is held constant, VA would also go up
- Any amount of breaths over 40, is just replacing dead space air, that is why people pass out when you have panic attacks
Explain the spirometry trend and components
-
Tidal Volume
- Volume of air during normal (quiet) breathing cycle (eupnea)
- ~500 ml
-
Inspiratory Reserve Volume
- Volume that can be inspired (over tidal) with maximum effort
- Hyperpnea
- 1500 - 500 ml
-
Expiratory Reserve Volume
- Volume that can be expelled (after tidal) with maximum effort
- 500 - 1000 ml
- Volume that can be expelled (after tidal) with maximum effort
-
Residual Volume
- Volume of air that remains in the lung, even after maximum exhalation
- Not normally measurable
- 900 - 1200 ml
- Due to surfactant, intrapleural pressure
- Volume of air that remains in the lung, even after maximum exhalation
-
Minimal volume (after collapse)
- 30 - 120 ml

Explain how each of the following are determined and if you can measure them
- Total Lung Capacity
- Inspiratory Capacity (IC)
- Vital Capacity (VC)
- Functional Residual Capacity
VT = Tital Volume
IRV = Inspiratory Reserve Volume
ERV = Expiratory Reserve Volume
Vres = Residual Volume
-
Total Lung Capacity = VT + IRV + ERV + Vres
- No, cannot measure Vres
-
Inspiratory Capacity (IC) = VT + IRV
- Yes, can measure
-
Vital Capacity (VC) = VT + IRV + ERV
- Yes, can measure
-
Functional Residual Capacity = ERV + Vres
- No, cannot measure Vres
Explain an overview of gas exchange?
-
Gas diffuses down its own concentration gradient
- usually talk in partial pressure gradient
- The structure of the respiratory memebrane is well adapted for the exchange of O2 and CO2
-
Hemoglobin carries both O2 and CO2
- Must have an affinity to oxygen but also needs to be able to dump it off
Explain the physics behind gas movement

Explain what makes up air and the details of partial pressure and dalton’s law
-
What is air?
- Mixture: N2, O2, H2O, CO2, other
- Partial Pressure = % air X air pressure
-
Dalton’s Law: PN2 + PO2 + PCO2 + PH2O = 760 mm Hg
- PO2 = 760 mm Hg (21%) = 160 mm Hg
- PCO2 = 760 mm Hg (0.04%) = 0.3mm Hg
Explain Henry’s Law
Amount of gas in a solution: is directly proportional to its partial pressure
-
Henry’s Law
- And depends upon the solubility of the gas
- CO2 is more soluble in water than O2

Explain alveolar gas exchange
Respiratory Efficiency
- Large partial pressure gradient
- Short distance
- High permeability
- Large surface area
- Greater blood flow around higher alveolar O2 levels and vice versa

Explain the oxygen hemoglobin saturation curve and the overall transport of Oxygen
Transport: O2
- Hemoglobin:
- Hb + O2 -><- HbO2
- Hemoglobin saturation
- % of heme units bound to O2
Transport based on the partial pressures in the blood and tissue as to where it is dropped

Explain the partial pressure differences in the circulatory system and how it impacts the respiratory system

Explain Alveolar capillary diffusion with CO2 and O2

Explain the Hemoglobin saturation curve impact with a change in pH
- Decreased acidity causes more O2 release
- (decreased affinity
- Bohr effect
- eg due to metabolism

Explain the hemoglobin saturation curve impact with a change in temperature
- Increased temperature causes more O2 release (decreased affinity)
- again, due to metabolism

Explain CO2 transport type
-
Bicarbonate Ions / carbonic acid
- ~90% of CO2 transported
- CO2 + H2O -><- H2CO3 -><- H+ + HCO3-
- Catalyzed by carbonic anhydrase
- converts the chemical reaction (no ATP)
- Exchanged for Cl- (chloride shift) = simporter
-
Bound to Hemoglobin
- ~5% of CO2, about 20% of the exchanged CO2
- CO2 + Hb -><- HbCO2
- Carbonimohemoglobin - attraction to CO2
-
Dissolved Gas
- ~5% of CO2, because CO2 is water soluble

Explain the systemic gas exchange process
-
Unloading of oxygen
- Diffusion (100 -> 40 mm Hg)
-
Loading of carbon dioxide
- Diffusion (46 -> 40 mm Hg)
Facilitating this shift is where bicarbonate ions are exchanged for Cl- ions
We load our tissue with tissues to allow for it to metabolize and produce energy for the cells

Explain a summary of respiratory control

Explain a summary of neural control of breathing

Explain Hemoglobin Saturation and curve
Arterial blood:
- PO2 = 100 mm Hg
- 98.5% saturated (hemoglobin not perfect)
Venous blood:
- PO2 = 40 mm Hg
- 75% saturated
Curve due to change in shape with O2 binding

Explain the positive feedback
Implications:
- Good saturation throughout normal body conditions
- Self-regulating system:
- As blood PO2 falls, more O2 is released
- Say, due to increased metabolism
- Oxygen stored even in venous blood

Explain RBC Metabolism
- 2, 3 BPG
- Produced by RBCs
- High altitude, anemia
- Decreases O2 affinity
- Curve shift?
Explain Fetal Hemoglobin shift
- Higher affinity for O2 Overall
- Steep slope means more sensitive O2 release

What are the overall functions of the digestive system?
Ingestion
Digestion (mechanical and chemical)
Absorption
Compaction
Defecation
What are the main conditions that affect hemoglobin saturation?
- PO2 of blood
- Blood pH
- Temperature
- RBC metabolism
What is oxyhemoglobin (HbO2)?
if one or more molecules of O2 are bound to hemoglobin, the compound is called oxyhemoglobin
Whereas hemoglobin with no oxygen bound = deoxyhemoglobin
A blood pH > 7.45 is called _____ and can be caused by a CO2 deficiency called _____
alkalosis, hypocapnia
- alkalosis = pH > 7
- Hypocapnia = most common cause of alkalosis, Pco2 < 37 mm Hg
What is the most common cause of acidosis?
Hypercapnia
Pco2 > 43 mm Hg
What is the thing that catalyzes the equation to make bicarbonate?
carbonic anhydrase
Name each of the accessory organs of the digestive tract and describe the function

Describe how the overall digestive system processes are accomplished
- Secretions
- By accessory glands
- Motility
- Skeletal muscles
- Smooth muscles
- Multi unit
- Visceral (single unit)
- Peristalsis = one direction
- Segmentation = bidirectional mixing

Describe the smooth muscles of the digestive system

Describe the overall digestive system histology
- Four layers:
- Mucosa
- Muscous membrane
- Lamina propria
- Submucosa
- Muscularis externa
- Serosa
- Mucosa

Describe the cellular level digestive system histology
Four layers:
- Mucosa
- Muscous membrane
- Lamina propria
- Submucosa
- Muscularis externa
- Serosa

what is the esophagus, stomach and intestine nervous system network called and what does it do?
enteric nervous system
regulates digestive tract motility, secretion and blood flow
Explain the types of control of the digestive system
-
Neural (long)
-
Sympathetic/parasympathetic division
- carry sensory signals from the digestive tract to the brainstem and motor commands back to the digestive tract (vagus nerves)
-
Sympathetic/parasympathetic division
-
Neural (short)
-
Enteric nervous system
- stretching or chemical stimulation of the digestive tract acts through the myenteric plexus to stimulate contraction
-
Enteric nervous system
-
Hormones
- gastrin and secretin
-
Local mechanisms, reflexes
-
secretions = histamine and prostaglandins
- stimulate movement
-
secretions = histamine and prostaglandins

Name the functions of the tongue
Manipulation
Sensation
Production of lingual lipase
(is a skeletal muscle)
What are the glands that make up your mouth region?
Parotid, sublingual, submandibular
What is the composition of saliva?
water, buffers, antibodies, amylase, mucin, urea
Explain salivary control
- Medulla oblongata (MO) salivary center (salivatory nuclei)
- Parasympathetic stimulation: lots of watery saliva
- Sympathetic inhibition: little, viscous saliva
- Response to stimuli
- Smell, taste or thought of food
Describe the pharynx
- Shared passageway (esophagus and trachea)
- Oropharynx
- Laryngopharynx
Explain the basics of the esophagus
muscular tube
Superior and inferior esophageal sphincters
Explain the phases of swallowing
-
Voluntary oral phase
- During chewing, tongue collects food and presses against palate and collects in oropharynx
-
Involuntary pharyngeal phase
- vocal folds and nasal cavity close to prevent food from going in the wrong place
-
Esophageal phase
- wave of involuntary peristalsis

What are the structures that make up the Lower GI Tract?
Stomach
Accessory Glands
Small intestine
Digestive Hormonal Regulation
Explain the cell in the stomach that specializes in cell replacement?
Stem cells
Explain the cell in the stomach that specializes in cell protection?
Mucous cell
Explain the cell in the stomach that specializes in the secretion of HCl, intrinsic factor, ghrelin?
Parietal cells
Explain the cell in the stomach that specializes in the secretion of pepsinogen?
chief cells
Explain the cell in the stomach that specializes in the secretion of chemical messengers?
Enteroendocrine cells
Explain a summary of the cellular specialization in the stomach
Stem cells: Replacement
Mucous cells: protection
Parietal cells: HCl, intrinsic factor, ghrelin
Chief cells: pepsinogen
Enteroendocrine cells: chemical messengers
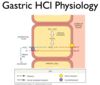
Explain the volume and types of gastric secretion
produce 2 to 3 L of gastric juice per day
-
HCl
- Mechanism:
- CO2 + H2O -> H2CO3 -> HCO3- + H+
- H+ / K+ pump
- Chloride shift
- Alkaline tide
- Functions:
- Antibacerial action
- Protein denaturation
- Cell wall breakdown
- Pepsin activation
- Mechanism:
-
Enzymes
- Pepsinogen to pepsin (protein digestion)
- Gastric lipase (Fats)
- Intrinsic factor (Vitamin B12 absorption)
- Chemical messengers
explain the gastric function in the stomach
- Distention stimulates churning
- Gastric emptying through pyloric sphincter
- (~3 ml per squirt)
- Time in stomach varies
- Digestion: proteins and fats
- Absorption: not much
Explain the cellular anatomy of the stomach

What are the three stages that make up the gastric activity?
- Cephalic phase
- Gastric phase
- Intestinal phase
Explain the cephalic phase of gastric functional regulation
- Cephalic Phase: (PREP PHASE)
- Stimulus: Sight, smell, taste of food
- Hypothalamus -> vagus nerve -> enteric NS
- Response: Gastric juice secretion, gastrin release

Explain the gastric phase of gastric functional regulation
- Gastric: WORK
- Stimuli: Distention, pH increase, Undigested proteins
- Response: Increased gastric juice secretion, gastrin release, increased churning

Explain the intestinal phase of gastric functional regulation
- Intestinal Phase: (CONTROL)
- Stimuli: Chyme in SI, pH decrease, Undigested nutrients
- Response: Hormone release, suppress gastric activity

Explain the summary of hormones in the lower GI track

Explain the liver overall anatomical structures, histology, and physiology
-
Anatomical overview:
- Four lobes
- Hepatic portal vein
- Hepatic artery
-
Liver histology:
- Lobules
- Blood and bile vessels
- Kupffer cells (in sinusoids)
- Macrophages (remove bacteria and debris from blood)
- Lobules
-
Liver Physiology
- Liver digestive function: bile production (fat emulsifier)

What is the function of the gallbladder?
storage of bile, release under control of CCK
Explain the general anatomy of the pancreas
Pancreatic ducts
Ampulla of Vader (hepatopancreatic)
Sphicter of Oddi
Explain the histology of the pancreas
- Endocrine
- Islets of Langerhans
- Insulin and glucagon - sugar level balance
- Islets of Langerhans
- Exocrin
- Acini cells: secrete pancreatic juice
- Neutralization
- Acini cells: secrete pancreatic juice

Explain the pancreatic physiological exocrine secretions
-
Exocrine secretions (Secretions that cut up carbohydrates, lipids and protein)
-
Enzymes (CCK controlled)
- All nutrient classes
- PSN (ACh from parasympathetic system), CCK regulate secretions
- All nutrient classes
- Bicarbonate (Secretion controlled)
-
Enzymes (CCK controlled)
Regulation of secretion:
-
ACh
- stimulates pancreatic acini to secrete their enzymes during cephalic phase
-
CCK
- response to fat in small intestine, stimulates pancreatic acini to secrete enzymes.
- Gallbladder release
-
Secretin
- response to acidity of chyme = neutralize
Explain the primary digestion and absorption of the small intestines, sections and surface area adaptations
Primary site of digestion and absorption
- Accepts secretions of the liver and pancreas
- Three sections:
- Duodenum, jejunum, ileum
- Ileocecal valve
- Surface area adaptations
- Plicae (circular folds)
- Villi
- Microvilli
Explain the histology of the small intestines
- Extensive capillary beds (absorbs everything but fat)
- Lacteal
- Duodenal (Brunner’s) glands
- Glands in the submucosa, mucus and alkaline secretions
- Mucus production
- Intestinal glands (crypts of Leiberkuhn)
- Brush boarder enzme production
Explain the intestinal motility
- Weak peristaltic waves:
- Local (myenteric) control
- Gastroenteric reflex:
- Whole intestine motility
- Gastroileal reflex:
- Relaxation of ileocecal valve
Explain the gastrin digestive hormonal regulation feedback loop
- Stimulus
- Food sensation (senses and distention)
- Sensors/CC:
- G cells in gastric pits
- direct and interic stimulation (vagus nerve)
- G cells in gastric pits
- Effectors:
- Gastric secretory cells
- gastric smooth muscle
- pyloric sphincter
- Response:
- Increased gastric activity and motility
Explain the CCK digestive hormonal regulation feedback loop
- Stimulus
- Lipid chyme in intestine (high fats)
- Sensors/CC:
- SI enteroendocrin cells
- Response:
- Gastric glands inhibited
- stimulates release in pancrease and gallbladder
- decreased hunger (CNS)
Explain the Secretin digestive hormonal regulation feedback loop
- Stimulus:
- Acid chyme in intestine
- Sensor:
- SI enteroendocrine cells
- Response:
- Pancreatic buffers and bile production/secretion
- Gastric glands inhibited
- Gastric motility inhibited (pyloric sphincter)
Explain the GIP (Glucose-dependent insulinotropic peptide) digestive hormonal regulation feedback loop
- Stimulus:
- Glucose hyperosmolarity
- Sensor:
- SI enteroendocrine cells
- Effectors/response:
- Islets of Langerhans - insulin secretion
Explain the VIP (Vasoactive intestinal peptide) digestive hormonal regulation feedback loop
- Stimulus:
- Distention of pylorus
- Sensors/CC:
- SI enteroendocrine cells
- Effectors/Response:
- Intestinal glands - increased secretion
- Vasodilation of intestinal vessels
- Gastric glands inhibited
Explain hydrolysis
water comes in, splits a molecule and results with a combining of one molecule with an OH and another with an H
Explain carbohydrate digestion enzymes and products
- Major enzymes:
- Salivary and pancreatic amylase (SUGARS)
- Products:
- Maltose (disaccaride)
- Limit dextrins (due to branching)
- Further digestion
- Intestinal brush boarder enzymes
Sucrase: Sucrose -> fructose + glucose
Maltase: Maltose -> 2 glucose
Lactase: Lactose -> galactose + glucose

Explain carbohydrate absorption
- Lumen -> blood
- Glucose and galactose:
- Na+ cotransport across apical membrane (SGLT transporters)
- Facilitated diffusion across basolateral
- Solvent drag (because glucose is highly soluble)
- Fructose
- Facilitated diffusion
- Glucose and galactose:

Explain the types of protein digestion
-
Endopeptidases
- Breaks interior amino acid bonds
-
Expeptidases
- Cleaves at ends (pac-man style)
-
Zymogens
- Produced in an inactive form
Explain protein digestion in the stomach
- Pepsin (endopeptidase)
- Produced as pepsinogen
- Secreted by chief cells
- Activated by acidity of stomach

Explain protein digestion in the small intestine
- Pancreatic proteases
- Trypsin (endo)
- Chymotrypsin (endo)
- Carboxypeptidase (exo)
- Brush boarder proteases
- Aminopeptidase (exo)
- Dipeptidase (endo)
- Enterokinase (activator)
- turns on trypsin

Explain protein absorption
-
Apical membrane
- Amino acids
- Na+ cotransport
- Amino acids
-
Dipeptides, tripeptides
- Active cotransport
- Broken down further inside cell
- infants can bring more into cell
-
Basolateral membrane
- Facilitated diffusion
- Lots of carrier proteins to allow things into the cell
- Facilitated diffusion

Explain lipid digestion and lipid packaging
- Issues:
- Hydrophobic
- Tendency to aggregate
- Bile (emulsification)
- Lipases:
- Lingual
- Pancreatic
- works on surface area, takes long time
- Lipase activity
- Triglycerides -> monoglyceride + 2 fatty acids
- Micelle
- Absorbable lipid / bile salt complex
- Lipid packaging
- Chylomicrons
- Triglyceride /cholesterol assemblies
- Chylomicrons

Explain lipid absorption
- Diffusion
- Reassembly
- Golgi chylomicron packaging
- exocytosis
- lacteal entry

Name and describe other nondigested things in the small intestine
-
Vitamins
- Fat soluble (A, D, E, K) absorbed with fats
- Water soluble via diffusion
- B12 -> intinsic factor
- Greatly enhances the absorption of Vitamin B12
-
Minerals
- Channel - mediated diffusion
- Na+, K+, Cl-, HCO3-
- Active transport
- Na+, Ca2+, Mg2+, Fe2+
- Cotransport
- Na+
- Channel - mediated diffusion
-
Water absorption
- Two liters consumed, but 7 liters enter GI tract
- Secretions: salivary, gastric, etc.
- Passive:
- Driven by osmotic gradient
- “water follows salt”
- Two liters consumed, but 7 liters enter GI tract
What are the functions of the large intestine
water absorption
Vitamin absorption
Production and elimination of feces
Explain the histology of the large intestine
- Lack of villi
- No enzyme production
- Numerous goblet cells (mucus producing)
Explain the physiology and reflex of the large intestine
- Absorption
- Water ~1 L daily
- Bacteria produced vitamins:
- K, biotin, B5
- Movement
- Haustral churning
- Mass movements
- Defication relex

Explain the long term and short term appetite regulation
-
Short-term regulation
-
Ghrelin
- Secreted by parietal cells when empty
- Stimulates feeding centers of hypothalamus
-
Peptide YY and CCK
- Secreted by enteroendocrine cells when chyme enters small intestine
- Inhibit feeding centers of hypothalamus
-
Ghrelin
-
Long-term Regulation
-
Leptin
- Secreted by adipose tissue when fat stores are ‘high’
- Stimulates satiety center (set point)
-
Insulin
- Inhibits feeding center (high blood glucose)
-
Leptin

Explain calories
- Usable energy sources when oxidized
- Fats: 9 kcal/g
- Carbs and proteins: 4 kcal/g
What are the macronutrients
- Carbohydrates
- Fiber
- Lipids
- Protein
Explain the macronutrient carbohydrate and the dietary sources
Stored, energy source, regulation, dietary source
-
Carbohydrates:
- 440 g stored: 434 g muscles, 100 g liver, 15-20 plasma
- Neurons and RBC exclusive energy source
- Regulated by insulin and glucagon
-
Dietary sources:
- Starches
- sugars
Explain the fiber macronutrient
cellulose
RDA 30 g/daily
Explain an overview of the Lipid macronutrient
- 15 - 25% of body weight
- 80 - 90 % energy requirement
- RDA < 30% calories from fat
What are the types of lipid transport?
-
Lipoproteins
- Protein + lipid transport
-
Chylomicrons
- small particle like micelle
-
VLDL
- very low density lipoprotein
- IDL
- LDL
- HDL
Explain the exogenous lipid pathway
Dietary source
- Digestive tract
- -> lymphatic system
- -> circulatory system
- -> tisues via lipoprotien lipase action
- Bypasses hepatic portal system
- Chylomicron fate
- Lipoprotein lipase
- Break down chylomicrons for fatty acid absorption

Explain the endogenous lipid pathway
Liver source
Liver -> VLDL -> IDL -> Tissue
- Chylomicron enters liver
- VLDLs formed -> circulation
- Muscles and fat cells absorb triglycerides
- teturn to liver as IDL

Explain cholesterol transport of lipids
- Low-density lipoprotien (LDL) formed
- Triglycerides removed
- Cholesterol added
- Released into circulation
- LDLs are cholesterol “deliveries”
- LDLs absorbed by tissues and broken down
- Excess cholesterol is released
- Absorbed by HDLs
Problem: if ICF cholesterol levels are high, LDLs NOT absorbed
- Statins decrease cholesterol production in liver
Explain protein macronutrient
RDA 0.37 x body weight (lb) in grams
Essential and inessential proteins
Name and describe the micronutrients
-
Minerals
- Function:
- Bones
- Molecular structure
- Electrolytes (Na+, K+, Ca2+, Cl-)
- Function:
-
Vitamins
- 13 essential organic compounds
- Metabolic constituents or precursors
- Fat soluble
- A, D, E, K
- Water soluble
- B-complex (8), C
Explain the difference between catabolism and anabolism
- Catabolism:
- Exergonic
- Energy yielding
- Anabolism:
- Endergonic
- Energy requiring

Explain cellular energetic (redox cycles), name and describe details of each cycle
-
Citric acid cycle:
- NADH and FADH2
- Acetyl CoA -> 3 NADH + 1 FADH2 + 2 CO2 + 1 ATP
-
Oxidative phosphorylation: (electron transport chain)
- ATP Production
- NADH / FADH2 oxidized -> H2O produced
- Energy lost to create the H+ gradient to allow for H+ to diffuse down ATP synthase and make ATP

Name and state anabolic or catabolic to the types of carbohydrate metabolsm
- Glycolysis (catabolic)
- Gluconeogenesis (anabolic)
- Glycogenlysis (catabolic)
- Glycogenesis (anabolic)

Explain Glycolysis carbohydrate metabolism
- Anaerobic in cytosol
- Glucose -> 2 pyruvate + 2 NADH + 2 ATP
- (if O2 present) Pyruvate -> acetyl CoA + CO2
- (If not) Pyruvate -> lactate

Explain gluconeogenesis carbohydrate metabolism
- Anabolic
- Glucose synthesis (ATP Required!)
- Precursors:
- Pyruvate
- Ketogenic amino acid
- Glycerol
- Lactate (cori cycle)

Explain glycogenolysis carbohydrate metabolism
- catabolic
- Glycogen -> glucose
- Glucagon and epinephrine stimulated (fight or flight response)
- Occurs in skeletal muscle and liver

Explain glycogenesis carbohydrate metabolism
- anabolic
- Glucose -> glycogen (stimulated by insulin)
- Medium term energy storage

Explain lipid metabolsms catabolic process
LIPOLYSIS
- Triglycerides -> fatty acids
- Beta - oxidation
- Fatty acids -> acetyl CoA (51 ATP per 6C)
- Excess -> acetone

Explain lipid metabolsms anabolic process
Lipogenesis
- Acetyl CoA -> fatty acids (glycolysis) -> glycerol -> triglycerides
- Because of the accumulation of ATP, does not go into mitochondria and the fat builds

Explain the types of protein catabolism metabolism
-
Transamination:
- Amino acid + keto acid -> new amino acid + new keto acid
- then enters citric acid cycle
-
Deamination:
-
Amino acid -> keto acid + ammonium ion
- Urea cycle
- If do not have any glucose or fats
-
Amino acid -> keto acid + ammonium ion

Explain protein anabolism metabolism
Amination or transamination of keto acids
(stick an amino group onto it, requires NRG)

Explain the nutrient metabolism summary

Explain the overall metabolism summary

Explain the absorptive state (after a meal)
Major process, primary fuel, controlling hormones
- Anabolism favored: Storing energy
- Building and storing (anabolic activities)
- Primary fuel: glucose
- Controlling hormone: insulin, enterohomones
- GRP and CCK also impact because food is being stored

Explain the absortive state (after a meal) pathway

Explain the postabsorptive state (between meals/starvation)
Major process, primary fuel, controlling hormones
- Catabolism: releasing energy
- Fuel source: mostly fatty acids
- Controlling hormones: Glucagon, epinephrine, growth hormone, glucocorticoids

Explain the post absorptive state pathway

Explain the metabolic rate
- Basal metabolic rate (BMR)
- Just enough energy to maintain vital function
- Caloric intake (Mifflin estimate)
- P=[10 x m (kg) + 6.25 x h (cm) - 5.0 x age + s] kcal/day
- s = +5 males, -161 females
- Does not take into account exercise, lean body mass
Explain thermoregulation
- Heat transfer
- Convection
- Radiation
- Evaporation
- Conduction
- Control:
- Hypothalamus
