L2: Shoulder Anatomy and Biomechanics Flashcards
What are the 5 functions of the shoulder?
- position the hand away from and towards the body
- provide us with an evolutionary advantage
- Load bearing – compression, traction
- Fastest joint in the body with rotation (9000o/sec)
- Greatest ROM in the body
What are 3 evolutionary advantages?
Compared to non-human primates, humans have a distinct evolutionary advantage:
- increased rotation ROM
- humeral torsion = increased ER
- more lateral orientation of the glenoid
This means that we have a greater capacity to throw
What is stability VS mobility in the UL?

What are 5 charcteristics of the shoulder complex?
- Multi-joint and multidirectional
- Need to consider major anatomical structures
- brachial plexus
- large vessels posterior to proximal clavicle
- Age changes
- Individual variation in structure and movement- Ranges of GHJ and scapula movements –> a lot of asymmetry
- Stability mechanisms
What are the 7 components of the shoulder complex?
- Glenohumeral joint (GHJ)
- Acromioclavicular joint (ACJ)
- Sternoclavicular joint (SCJ)
- Scapulothoracic joint
- Thoracic spine
- Cervical spine
- Lumbar spine

What are 5 components that are involved in elevation?
- Scapulothoracic joint
- Glenohumeral joint
- Clavicle (ACJ, SCJ)
- Thoracic spine
- Lumbar spine & pelvis
TrA activates first in shoulder flexion –> whole body activation

What does the suprascapula nerve (C5,6) innervate? Where does it travel?

What does the suprascapula nerve (C5,6) innervate? Where does it travel?
- Originates from the superior trunk of the brachial plexus
- Passes through the suprascapular foramen to reach the posterior scapula, where it lies in the plane between the bone and the muscle
- Innervates supraspinatus, then passes through the greater scapular notch (between the root of the spine and the glenoid cavity) to terminate in and innervate the infraspinatus
- Generally has no cutaneous branches

Which area on the suprascapular nerve is most commonly impinged?
Greater scapular notch
What does the axilliary nerve (C5,6) innervate? Where does it travel?
- Originates from the posterior cord of the brachial plexus
- Passes inferiorly & laterally along the posterior wall to exit the axilla through the quadrangular space, then passes posteriorly around the surgical neck of the humerus
- Innervates deltoid and teres minor
- Branches into superior lateral cutaneous nerve (loops around posterior margin of deltoid to innervate skin in that region)
- Accompanied by posterior circumflex humeral artery

What does the accessory nerve (CN XI) innervate? Where does it travel?
Innervates trapezius and sternocleidomastoid (with contributions from cervical plexus C2-4)

What does the long thoracic nerve (C5,6,7) innervate? Where does it travel?
Innervates serratus anterior
Traction injury –> winging of medial border

What does the dorsal scapular nerve (C4,5) innervate? Where does it travel?
Innervates rhomboid major, rhomboid major, and levator scapulae

The shoulder is a remarkable complex, but there is a trade off
between____ and _____.
mobility; stability
The shoulder complex consists of the ____, ____, ____ and
_____ joint… but also need to consider the thoracic spine, cervical spine,
lumbar spine and pelvis
GHJ, ACJ, SCJ, scapulothoracic
The shoulder is highly innervated… need to be aware of nerves as a source of ____ and ____ , as this has implications for management
pain; dysfunction
What are 6 characteristics of sternoclavicular joint?
- Only articular attachment of the shoulder girdle to the axial skeleton
- Costoclavicular and capsular ligaments
- Movement: rotation and translation (AP, sup/inf)… clavicle on the articular disc moves more than disc on the sternum
- Close to rib 1
- Neurovascular bundle
- Subclavius muscle

What are 2 injuries with the sternoclavicular joint?
- posterior dislocation (direct force e.g. MVA, sport) – emergency
- Can get arthritis or injury to ligament
- anterior dislocation (indirect force e.g. fall on shoulder)
- Due to neurovascular bundle

What are the 3 mechanical movements of the sternoclavicular joint?

What are 3 characteristics of the acromioclavicular joint?
- Plane type synovial joint between distal clavicle and acromion
- Movement: accessory (elevation/depression; forward/backward shear)
- Scapula rotates at the ACJ
What are 3 passive supports from ligaments in the ACJ?
- Acromioclavicular
- Coracoclavicular
- Trapezoid
- Conoid
- Coracoacromial ligament
What are 2 dynamic (indirect) support from muscles in the ACJ?
- Deltoid
- Upper trapezius

What are 3 steps that occur during arm elevation in the ACJ mechanics?
- Clavicle elevates distally and retracts and rotates posteriorly
- 30o of elevation occurs at the ACJ
- 15o early in movement
- 15o after 135o of arm elevation
- Minimal movement of the clavicle between 90-135o

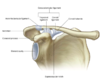
What are 2 characteristics of the GHJ?
- Joint with the largest ROM in the human body… BUT sacrifices stability for mobility
- Large ball and smaller pearshaped socket (disproportionate)

What are the GHJ mechanics?

What is the GHJ at the end of range?
most stability comes from capsuloligamentous structures
What is the GHJ through range?
- capsule relaxed
- most stability comes from muscle
What are 6 structures contributing to passive stability in the GHJ?
- glenoid orientation
- surface tension
- negative intra-articular pressure
- labrum (fibrous)
- capsuloligamentous structures
- osseo-ligamentous coracoacromial arch (superior)
What are 2 structures contributing to dynamic stability in the GHJ?
- rotator cuff
- scapular orientation (dynamic control of glenoid position)
What are 3 characteristics of the concavity of glenoid fossa (GHJ passive stability)?
- retroverted 7o (posterior facing), upwardly tilted 5o
- if glenoid fossa is anteriorly tilted, increased risk of instability
- position of glenoid largely driven by position/control of the scapula

What are 2 characteristics of the surface tension (GHJ passive stability)?
- cohesive bond between joint surfaces, limiting free fluid movement
- allows translation but prevents distraction

What is a characteristic of the negative intra-articular pressure (GHJ passive stability)?
Draws capsule inward & tightens fibres

What are 5 characteristics of the labrum (GHJ passive stability)?
- made of pliable fibrocartilage
- blends with long head of biceps (LHB) and superior glenohumeral ligament (SGHL)
- deepens socket by 50%
- 25% of humeral head contacts glenoid
- 75% of articular surface of humeral head is in contact with labrum & glenoid
- provides stability in mid-range
- nociceptive nerve supply

What are the 6 capsuloligamentous structures of the GHJ?
- Coracoacromial ligament
- Coracohumeral ligament
- Transverse humeral ligament
- Superior GH ligament
- Middle GH ligament
- Inferior GH ligament
What are 4 characteristics of the coracoacromial ligament?
- base of the coracoid process & acromion
- strong triangular band
- restricts upward displacement of humeral head
- sits above the subacromial bursa

What are 4 characteristics of the coracohumeral ligament?
- supports dependent arm (limits inferior translation of adducted arm)
- restrains ER < 60o abduction
- restricts flexion & extension
- tunnel for LHB

What are 2 characteristics of the transverse humeral ligament?
- between greater & lesser tubercles of humerus
- holds LHB tendon in the intertubercular sulcus

What is a characteristic of the superior GH ligament?
blended with coracohumeral ligament
(although separated in images)

What are 2 characteristics of the middle GH ligament?
- superomedial margin of the glenoid cavity to the lesser tubercle
- greatest variation in size
What are 2 characteristics of the inferior GH ligament?
- anterior and posterior bands; axillary pouch
- inferiorly related to anatomical neck of humerus

What are the 4 positions that the anterior GH ligaments become taut?
- extension
- horizontal extension
- abduction and/or
- external rotation
Different components restrict movement in different positions

What is the anterior stability of the GHJ?

What are 4 passive structures that provides superior stability on the GHJ?
- coracohumeral ligament
- superior GH ligament
- rotator interval
- anterior superior aspect of the GHJ capsule, in the gap between subscapularis and supraspinatus; region where the capsule is reinforced by the coracohumeral ligament & superior GH ligament, & covered by LHB tendon
- acts as anterior superior hammock, restricts ER & inferior translation with arm by side
- orientation of glenoid

What are 2 dynamic structures that provides superior stability on the GHJ?
- rotator cuff (especially supraspinatus)
- deltoid

What are 2 passive structures that provides posterior stability on the GHJ?
- posterior capsule
- posterior band of inferior GH ligament

What a dynamic structure that provides posterior stability on the GHJ?
posterior rotator cuff

What are 4 positions that restrains the GHJ (posterior stability)?
- flexion
- abduction
- horizontal flexion
- internal rotation

What are 6 characteristics of the rotator cuff (dynamic stability)?
- reinforces (blends) capsule through tendinous attachments & increases tension in capsular ligaments
- centres humeral head on glenoid; force couple to prevent upward translation (e.g. with deltoid contraction)
- maintains joint compression between surfaces
- strength ratio:
- concentric ER/IR ratio in control participants (isokinetic dynamometry- Stronger inxto IR than ER):
- 60-70% in most testing positions (including 0o and 90o of abduction in the scapular plane)
- scapula position (Anteriorly tilted and downward tilted) can influence RC function
- intrinsic vs. extrinsic weakness:
- intrinsic: pain, weakness
- extrinsic: lack of stable base, or decreased facilitation by proximal muscle activation patterns
What does GHJ dynamic stability?

What are 9 characteristics of the rotator cuff: infraspinatus and teres minor (GHJ- dynamic stability)?
- transverse force couple with subscapularis (to control anterior translation)
- externally rotate GHJ
- resist superior and anterior humeral head translation
- depress the humeral head (with latissimus dorsi) – may be important to prevent impingement
- deceleration (eccentric)
- extend GHJ, especially at 90o abduction
- infraspinatus generates greatest torque at 0o abduction (e.g. shoulder ER in side lying)
- adding a rolled towel increases infraspinatus and teres minor EMG activity
- ER at 90o abduction increases supraspinatus
- and deltoid activity (Reinold et al 2009)

What are 6 characteristics of the rotator cuff: subscapularis (GHJ- dynamic stability)?
- reinforces the inferior capsule of the abducted shoulder
- transverse force couple with infraspinatus and teres minor (to control anterior translation) –> prevent posterior instability
- significant dynamic stabiliser to prevent
- posterior instability
- upper and lower portions function differently:
- When moving from 0-90o abduction, EMG activity of upper subscapularis either remained the same or decreased; EMG activity of lower portion increases
- internal rotator; resists ER
- in athletes, changes in EMG activity in the presence of pain (e.g. during rapid shoulder external rotation movement)- Pain can cause impaired dynamic control

What are 6 characteristics of the rotator cuff: supraspinatus (GHJ- dynamic stability)?
- compresses GHJ (especially during initiation of abduction)
- abductor
- generates small ER torque
- activity increases as resistance increases– peaks at 30-60o abduction / scaption
- greatest torque when shoulder is in neutral rotation
- less mid/post deltoid activity when perform ‘full can’ exercise in standing, v.s. ‘empty can’ or prone horizontal abduction with full ER

What are 3 characteristics of the rotator cuff: long head of biceps (GHJ- dynamic stability)?
- compresses GHJ
- enhances anterior stability
- important in acceleration and deceleration phases of throwing
Biceps tendon = intra-articular

The SCJ and ACJ are important contributors to ____ movement
shoulder
The GHJ relies on ____ and ___ structures for stability
… implications for managing patients with shoulder conditions
passive; active
The scapulothoracic joint is the ____ ‘joint’.
functional

What are the 2 things that scapular position is affected by?
- thoracic cage
- dynamic restraints

What are 2 reasons why scapular control is essential for robust SHJ stability?
- rotator cuff muscles attach to the scapula
- scapula position determines the orientation of the glenoid fossa

What are the 2 key influences on shoulder from impingement, stability?
- Influence on neural tissues – brachial plexus
- Influence on cervical spine – concurrent pathology

What are 6 characteristics of the resting position of the scapula?
- Sits between T2 & T7
- Flat against thoracic spine
- Anterior tilt ~5-8o
- 30-45o anterior to the coronal plane (scaption)
- Glenoid fossa is ~7o retroverted relative to the scapula, 5o upward tilt
- Asymmetry is normal… but may not be ideal

What are the 3 planes of rotation in scapular kinematics (scapulothoracic joint mechanics)?
- Upward, downward
- Anterior, posterior
- Internal, external

What are the 2 translations in scapular kinematics (scapulothoracic joint mechanics)?
- Elevation, depression
- Retraction, protraction

What are 2 characteristics of lower trapexius and serratus anterior (scapulothoracic joint mechanics)?
- produce posterior tilt, ER & upward rotation of the scapula
- prevent winging of the scapula (lower trapezius- inferior angle and serratus anterior- medial border)
What is the implication of an impingement/problem with lower trapexius and serratus anterior?
anterior tilt and downward
What is a characteristic of upper trapezius (scapulothoracic joint mechanics)?
produces upward rotation at the scapular spine

What is a characteristic of middle trapezius (scapulothoracic joint mechanics)?
produces upward rotation and external rotation

What is the force couple to initiate scapular motion (scapulothoracic joint mechanics)?
- Upper trapezius: upward rotation
- Serratus anterior: external rotation to maintain medial border against chest wall

What is the force couple to control elevation (scapulothoracic joint mechanics)?
Lower trapezius: upward rotation and posterior tilt to hold inferior angle against chest wall

What is the scapulothoracic joint mechanics for upper trapezius, lower trapezius and serratus anterior?
Maintain on chest wall and rotates upwards (elevation) 60% is through scapular not GHJ

What is the force couple to control end of range elevation (scapulothoracic joint mechanics)?
- Middle trapezius: upward rotation and external rotation
- Serratus anterior: external rotation to maintain medial border against chest wall
What are the 2 thoracic spine’s influences on the scapula complex (esp. scapula) in arm elevation?
- Bilateral = thoracic extension
- Unilateral = thoracic rotation
What are the 2 thoracic spine’s influences on the scapula complex (esp. scapula) in static posture?
- Kyphotic
- Flat / lordotic
What are the 2 thoracic spine’s influences on the scapula complex (esp. scapula) in dynamic posture?
- Hypermobile – move into thoracic extension
- Hypomobile (stiff) – stay in kyphosis
What are the 2 normal functions of the shoulder in terms of the scapula?
- stable base for upper limb movement
- important contribution to shoulder range of motion
Scapular muscles need to be functioning _____ (force couple) …implications for rehabilitation of patients with shoulder & other
upper limb conditions
optimally
What are the 4 characteristics of phases of upper limb elevation (flexion and abduction)?
- ~120o movement at the GHJ
- ~60o movement at the ACJ and SCJ (i.e. scapular movement)
- Humeral head is stabilised in the glenoid against upward translation by deltoid
- by transverse force couple(infraspinatus/teres minor + subscapularis)
- Rotation ROM is greatest in 0o and least in elevation

What are the 3 characteristics of the phases of upper limb elevation (0-60 degrees)?
- Primarily glenohumeral motion
- Small amount of upward scapular rotation
- Muscle activity
- Supraspinatus compresses humeral head into glenoid
- Deltoid muscle causes superior movement of head of humerus
- Infraspinatus, subscapularis and latissumus dorsi counter upward pull of deltoid

What are the 3 muscle activities in the phases of upper limb elevation (0-60 degrees)?
- Supraspinatus compresses humeral head into glenoid
- Deltoid muscle causes superior movement of head of humerus
- Infraspinatus, subscapularis and latissumus dorsi counter upward pull of deltoid

What are the 4 characteristics of the phases of upper limb elevation (60-140 degrees)?
- Upward rotation and posterior tilt of the scapula
- Near equal scapular and humeral movement
- Upward shearing force via deltoid reaches maximum at 60o
- Upward force counteracted by rotator cuff muscle activity

What are the 3 characteristics of the phases of upper limb elevation (140-180 degrees)?
- Upward rotation and external rotation of the scapula
- Humeral movement is 4x that of scapular movement
- Extensibility of teres minor and subscapularis allows maximal humeral movement on the scapula

What are the 4 characteristics of the phases of upper limb elevation (scaption)?
- Elevation of the arm 30o anterior to the frontal plane
- Length-tension relationship of abductor and rotator muscles suggested to be optimal
- Glenohumeral joint capsule is under less tension which facilitates movement
- Possible increased glenohumeral joint congruity and robust control of motion

What are the 2 characteristics of horizontal flexion/adduction?
- Increases stress on the ACJ
- Tensions posterior capsule

What are the 3 characteristics of hands behind head, hand behind back?
- Combined movements
- HBH: abduction, flexion, ER
- HBH: adduction, extension, IR
- Useful screening movements in assessment
- Replicate function

Different components of the shoulder complex contribute to
different phases of_____.
elevation
Different muscles contribute to motion and stability during different phases of ______ and there are implications for assessment and optimal rehabilitation of patients with shoulder problems.
elevation
