L16 Benzodiazepines + Antiolytics Flashcards
Learning Outcomes (for general perusal)
- Describe the essential features of the main mental illnesses in which BDZ are indicated
- Describe the location and function of the principal neurotransmitters involved in the action of benzodiazepines.
- Describe the mechanisms of action, desired effects and principal adverse effects of benzodiazepines (BDZ): anxiolytics and hypnotics
- Relate the mechanisms of tolerance and dependence of anxiolytics to restrictions of their clinical use.
What is anxiety?
A feeling of worry, nervousness, or unease about something with an uncertain outcome (normal)
A nervous disorder marked by excessive uneasiness and apprehension. (pathological)
What are the symptoms of anxiety?
- Cognitive Beliefs -inability to cope with stress, unrealistic ideas of danger
- Emotional - feelings of fear, apprehension, irritability, low mood
- Somatic Symptoms -hyperventilation, retrosternal constriction, muscle tension, autonomic overactivity
- Behavioural - reduced purposeful activity, increased purposeless activity, avoidance.
- Arousal - increased alertness, hypervigilance, restlessness
What are the different types of anxiety?
- Normal
- Trait Anxiety
- Anxiety Disorders
- Situational Anxiety
- Secondary to drug withdrawal
- Secondary to drug use
- Secondary to other psychiatric illness
- Secondary to physical illness
How does anxiety show Psychic/Somatic interaction?
Cannon (1915) considered the emotional experience to be primary, i.e. the bodily change is caused by the emotion.
- An example is the ‘fight or flight’ response to a threat.
- In this a major role is subserved by the autonomic nervous system in preparing the organism to respond.
Papez (1937) identified a ‘circuit’ of brain regions which subserve emotional expression. These are part of the limbic system.
What are the Biological Theories of Anxiety Disorders?
Focus on last one
BRAIN AREAS
- Periaqueductal grey area
- Medial hypothalamus
- Amygdala
- Septo-hippocampal system; -Temporal Cortex
NORADRENALINE
- LC stimulation in animals
- Effects of β-adrenoceptor antagonists
- Effects of α2 antagonists (yohimbine).
SEROTONIN
- Involved in brain aversion system
- benefits from 1A partial agonists & SSRIs.
GABA
- agonists reduce anxiety
- antagonists increase anxiety (e.g. pentylenetetrazol)
- gamma-2 knockout mice.
Name the drugs used in the treatment of anxiety disorders
- BENZODIAZEPINES
- BETA-ADRENOCEPTOR ANTAGONISTS
- SSRI ANTIDEPRESSANTS
- 5-HT-1A AGONISTS
- LOW DOSE ANTIPSYCHOTICS
- NEW APPROACHES (antagonists for CCK-B, CRF and Substance P; pre-gabalin)
Benzodiazepines
- Where is the specific binding site for BDZs?
- What does GABA act as in the CNS?
- What is the mode of action of BDZs?
- What occurs if GABA is absent or the R is blocked?

- In the GABA-A receptor in the GABA-BDZ Receptor Complex. (Junction between G2 and A1)
- An inhibitory transmitter
- When a BDZ occupies its own receptor it enhances the action of GABA at its receptor resulting in greater flow of ‘negative’ Clˉ ions into the neurone.
- Act on RAS -reticular activating system
- Act on limbic system of cortex – emotion
- BDZ on it’s own will have no effect

What are the clinical effects of BDZs?
- anxiolytic e.g. anxiety disorders, premedication,
- hypnotic e.g. sleep disorders
- anti-convulsant e.g. epilepsy
- muscle relaxant e.g. musclespasticity, myoclonus
BDZ : Pharmacokinetics
- How can they be given?
- When is peak plasma concentration reached?
- In what form are they in the blood?
- What causes them to accumulate in body fat?
- What are they metabolised to?
- What are they conjugated with in the liver?
- Well absorbed when given orally (almost complete bioavailability with oral dose), can also be given IV, IM, PR
- Within 1 hour (oxazepam absorbed more slowly)
- Bind strongly to plasma proteins
- High lipid solubility
- Active metabolites so half life doesn’t ways reflect the duration of action (e.g. diazepam - active metabolite n-desmethyldiazepam which has a half life of 60 hours) - must be careful not to overdose
- glucuronic acid
BDZs
Can be split into (short, med and long acting)
Give an example of each of the following, and a clinical use:
- Short-Acting BDZ
- Long-Acting BDZ
- BDZs which have anticonvulsant activity
- temazepam, lorazepam - hypnotics, reduced hangover effects
- diazepam, chlordiazepoxide - anxiolytic, anticonvulsant
- Rectal diazepam, IV diazepam
Name some general problems of BDZ use
- tolerance to the effects
- physical dependence
- psychological dependence
- active metabolites - prolonged effects
BDZ : Adverse Effects
- What are the toxic effects from BDZ overdose
- What are the unwanted effects during normal therapeutic range?
- When will tolerance and dependence begin to become evident? Why?
- Respiratory depression, prolonged sleep
- drowsiness, dizziness, dry mouth, blurred vision, ataxia, amnesia
- after two weeks - due to a change at receptor level
What are the features of BDZ withdrawal syndrome?
- Anxiety: sleep disturbance, sweating, tremor, dysphoria
- Disturbance of Perception: Hypersensitivity to stimuli, visual disturbance, depersonalisation, sense of body sway
- Rare: Paranoid Psychoses, Seizures, Depressive Illness
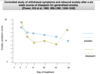
Withdrawal from long-term BDZ treatment
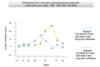
Withdrawal Symptoms and Rebound Anxiety
What are the stages of sleep?
- I (5%) - drowsy, shallow sleep - slow rolling eye movements
- II (50%) - Asleep - no eye movements, decreased muscle tone, HR and RR
- III (8%) - Asleep (slow wave sleep) - As for stage II
- IV (12%) - Asleep (slow wave sleep) - As for stage II
- REM (25%) - Dreaming - Bursts of rapid eye movement, increased cerebral blood flow, HR, RR and BP are all very variable

BDZ as Hypnotics
- What does insomnia involve?
- What do hypnotics do?
- What characteristics does drug-induced sleep have?
- What to BDZ do?
- What is a benefit?
- initial insomnia and early morning wakening
- induce sleep, treat insomnia in the short term if non pharmacological methods have failed
- Reduced REM component
- •BDZ reduce the time taken to get to sleep and increase the total duration of sleep in those who sleep <6 hours.
•Avoid hangover effect with those benzodiazepines with a short duration of action e.g. temazepam
- Don’t cause REM rebound that occurs with other hypnotics (nightmares)

