Imaging the Emergency Patient Flashcards
what are common traumatic injuries (6)
- pneumothorax
- pulmonary contusion
- pleural effusion (fluid)
- ascites
- diaphragmatic rupture
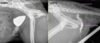
- fracture/luxations
identify the normal structures of the thorax (7)

- trachea
- cranial vena cava
- main stem bronchi
- bronchi
- pulmonary vessels
- caudal vena cava
- diaphragm
what are the criteria of imaging modalities (5)
- readily available
- conscious or mild sedation
- rapid
- minimal stress/not invasive
- easy to interpret (quality of image)
what are the prioritized areas
- thorax
- abdomen
- spine
- head
- limb
what is the effect of over exposure
too dark
lack of contrast
misdiagnose a pneumothorax
what are the effects of under exposure
too white
too little differentiation
misdiagnose abdominal fluid
what are anatomic artefacts
skin fold/lines

what should you normally see in the thorax (5)
- heart
- diaphragm
- trachea
- lungs (blood vessels)
- thoracic wall (ribs, sternum, vertebrae)

what should you look for to identify abnormalities
- loss of normal structure
- loss of normal architechture
what are traumatic lesions that can happen in the thoracic wall (4)
- diaphragmatic rupture
- fractured ribs
- fractured or dislocated sternum
- flail chest
what are some traumatic lesions that occur to the intrathoracic cavity (6)
- pneumothorax
- pulmonary contusion
- pneumomediastinum (cervical, pharyngeal?)
(1-3 more common)
- pleural effusion (hemothorax, chylothorax)
- cardiac tamponade (pericardial effusion)
- lung lobe torsion
(4-6 less common)
how does a pneumothorax present on radiograph (3)
- heart raised from sternum
- retraction of lung lobes –> free gas between lung and thoracic wall & loss of vascular markings peripherally
- increased lung opacity

what is occuring here

pneumothorax
what is occuring here

pneumothorax
free gas with no pulmonary markings
what are lung bulla/blebs

permanent air filled space within the lung –> lung trauma not clinically significant but if pop can lead to development of pneumothorax
what are the signs of a tension pneumothorax (4)
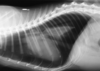
- heart raised from sternum
- retraction of lung lobes –> loss of vascular markings peripherally
- diaphragm pushed caudally –> diaphragm flat or concave
- increased intercostal spaces
what is a tension pneumothorax
air pressure is continually increased that can be developed in the lung paranchyma emergency
diaphragm flattened appearance
rounded chest
very poor gas exchange –> imminent danger for animal
what is the appearance of pulmonary contusions

lung has soft tissue opacity –> blood, edema
commonly seen but not always with pneumothorax
what is shown here

pulmonary contusion
how does pleural effusion appear on radiograph
- loss of cardiac shadow (DV, lateral if marked/severe effusion)
- retraction of lung lobes (soft tissue opacity in pleural space, outlines lungs, interlobar fissures, leaf or scalloped edges)
what is shown here

pleural effusion
may see faint lines running between intercostal spaces
how does a diaphragmatic rupture show on radiograph (6)
- can’t see diaphragm
- gas filled tubes of intestines in thorax
- abdomen is missing small intestine loops –> empty abdomen
- displaced/absent falciform fat
- cranial displacement of pylorus
- loss of diaphragmatic line
+/- pleural effusion
what is shown here
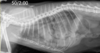
diaphragmatic rupture
how does pneumomediastinum show on radiograph
- visible contents of mediastinum
may track under skin
- tracheal/esophageal perforation
- cervical/pharyngeal wound
air building up in mediastinum space –> increased visibility of structures here (vascular structures)