GI Session 2 Flashcards
(23 cards)
Describe the protective role of saliva
To protect the oral environment. The oral environment is a complex one which needs to be protected. The oral mucosa and teeth are vulnerable to physical and chemical damage, and to infections. The saliva ensures a moist, chemically appropriate environmental with healthy bacterial flora.
- The mucosa, which is not cornified, must be kept wet.
- Teeth are constantly at risk from bacterial acid, which needs to be neutralized (saliva maintains alkaline environment) – saliva washes teeth
- High calcium concentration – protects teeth
- The bacterial ecology of the mouth needs to be maintained by mild bactericidal action (so healthy bacterial flora dominate and overwhelm pathogens).
What other roles does saliva have apart from protection?
- Saliva moistens and lubricates food
- Physical disruption of food is by mastication (chewing). Powerful muscles, mainly the Masseter muscle, innervated by a branch of the trigeminal nerve (cranial nerve 5), generate huge forces transmitted to food via the teeth. The incisors cut food into pieces and the molars crush it and mix it with saliva to form a paste which can be swallowed.
- The bolus is moistened and lubricated by saliva.
- Saliva also contains enzymes, which begin the digestion of (particularly) carbohydrates. NOT VERY SIGNIFICANT FUNCTION.
What is Xerostomia?
we can eat without saliva provided food is moist but if there is no secretion, the mouth very rapidly deteriorates. Teeth and mucosa can degrade very quickly, within weeks, to the acidic environment. Xerostomia could be due to malignancies affecting saliva glands. ‘Dry mouth’
Name the components of saliva
- We produce ~1.5L every day
- Hypotonic (i.e. excess water over other body fluids).
- Relatively low concentrations of Na+ and Cl-
- Excess concentration of K+, Ca2+ and I_
- I- is a bacteriostat – controls bacterial population in such a way that it maintains healthy flora
- Although resting saliva is neutral, once stimulated it becomes alkaline (HCO3- concentration is higher than plasma)
- Bacteriostats (so that pathogens aren’t overwhelmed; conditions favour healthy flora
- Enzymes – salivary amylase
- SIGNIFICANT MUCUS content (mixture of mucopolysaccharides – coats and sticks to bolus, making it slippery)
Describe the salivary glands and their secretions
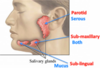
Saliva is secreted from 3 pairs of ducted, exocrine salivary glands:
- The parotid glands (get really big in an alcoholic) secrete about 25% of saliva by volume, and their secretion is SEROUS with a mixture of water, electrolytes and enzymes. Watery and rich in enzymes but little mucus.
- The sublingual glands secrete about 5% of saliva by volume, but their viscous secretion is rich in mucus, no enzymes and is therefore known as mucous saliva. The secretion contains relatively little water.
- The submandibular glands secrete about 70% of saliva by volume and secrete both serous and mucous components
-Gland is made of up of mixture of serous and mucus acini leading to common ducts.
What are the salivary glands composed of?
Salivary glands are composed of numerous blind-ended tubes with acini (lined with acinary cells) at the blind end and a connected system of ducts converging to outlets (rest of tubes are lined by duct cells with each tube having a single outlets) in the mouth.
- Serous acini are different in structure to mucus acini and the submandibular glands have a mixture of the two types
Explain the mechanisms of secretion of serous saliva
Saliva is always hypotonic to plasma but this cannot be achieved by pumping water directly. The hypotonicity is created by first secreting an isotonic (concentrated) solution and then removing ions from it.
Acinar cells secrete a fluid isotonc with ECF
- [Na+], [K+] about the same
- [I-] (iodide – greater)
- [Cl-] slightly less
- [HCO3-] about the same
- Enzmes
Ductal Modification: Duct cells then remove Na+ and Cl-, and add HCO3-.
- little change in volume
- [Na+] and [Cl-]
- [K+] rises somewhat
- NB: [HCO3-] falls hwne resting
The gaps between duct cells are tight, so water does not follow the resulting osmotic gradient, and saliva remains hypertonic.
At low flow rates, the duct cells remove most sodium, so saliva is very hypotonic. The capacity of duct cells to modify saliva is however limited, so at high flow rates a smaller fraction is removed and saliva becomes less hypotonic (less modified except for HCO3-) though the stimulus to secretion promotes HCO3- so saliva becomes more alkaline.
Describe the composition of Resting Saliva
- highly modified acinar secretion
- Low volume
- Very hypotonic ([Na+] 7-10mmol/l, [K+] c20mmol/l)
- Neutral or slightly acid (food which is acidic, and bacterial acid stimulate ductal cells to add HCO3-)
- Few enzymes
Describe the composition of stimulated, excited saliva
- less modified acinar secretion
- High volume
- Less hypotonic ([Na+] up to 80 mmol/l, [K+] 8-10mmol/l
- More alkaline (massive increase of [HCO3-] 50-60mmol/l)
- Lots of enzymes
What are the mechanisms of acinar secretion and ductal modification?
Mechanisms of Acinar Secretion:
- Cl- ions are actively secreted from acinar cells into the lumen of the duct.
- Water and other ions (Na+) will then follow passively.
Mechanisms of Ductal Modification:
- The action of Na+/K+-ATPase Antiporter in the basolateral membrane of duct cells lowers the [Na+] inside the cell. This means there is a concentration gradient where [Na+] is high in the duct lumen and low in the duct cells. Na+ diffuses passively back into the Duct cells.
- The action of the Na+/K+ also increases the [K+] inside the cell. The resulting concentration gradient drives the expulsion of Cl- from the duct cells into the ECF. Again, a concentration gradient is set up between the duct lumen and cells with [Cl-] low inside and [Cl-] high outside. The gradient drives the expulsion of HCO3- into the duct lumen.
- Membrane between Duct cell and ECF is known as basolateral membrane
- Duct is where the saliva is.

Describe the control of salivary secretion
- The volume of salivary secretion is controlled by the activity of acinar cells and the composition of salivary secretion is affected by duct cells.
- Salivary secretion is mostly controlled by the autonomic nervous system.
Describe the autonomic control of salivary secretion
Parasympathetic nerves from the otic ganglion stimulate acinar cells to increase primary secretion and duct cells to add extra HCO3- to saliva.
- Paratid gland is supplied by the Glossopharyngal Nerve (9th cranial nerve) from the otic ganglion.
- Submandibular and sublingual glands are supplied by the Facial Nerve (7th cranial nerve) from the submandibular ganglion.
Muscarinic receptors which are blocked by atropine-like drugs
Co-transmitters stimulate extra blood flow.
Salivary volume therefore depends on autonomic control. Autonomic outflow is coordinated from centres in the medulla of the brain stem in response to afferent stimuli from mouth and tongue in particular taste receptors especially acid, nose, conditioned reflexes (think Pavlov’s dogs)
Sympathetic nervous activity reduces blood flow to the salivary glands, which limits salivary flow, producing the typical dry mouth of anxiety – from the superior cervical ganglion.
What are the effects of parasympathetic outflow? What’s the effect of Aldosterone?
Parasympathetic outflow:
- Releases acetyl choline
- Acts on acinar cells to promote formation of primary secretion
- Duct cells to promote HCO3- secretion
The rate of ductal recovery of Na+ is increased by the hormone aldosterone from the adrenal cortex. Aldosterone increases the activity of ENaC and Na+/K+/ATPase, making saliva even more hypotonic.
Describe the oropharynx
The oropharynx lies behind the oral cavity and forms the portion of the pharynx below the nasopharynx but above the laryngopharynx. It extends from the uvula (extension at the back of the soft palate), to the level of the hyoid bone.
- Because both food and air pass through the oropharynx, a flap of tissue called the epiglottis closes over the glottis to prevent aspiration.

Describe the structure of the oesophagus
The oesophagus is a fibromuscular tube that passes food from the pharynx to the stomach. It is continuous with the lower part of the laryngopharynx. The oesophagus has several layers from inside to out:
- Mucosa composed of non-keratinized stratified squamous epithelium, lamina propria and a layer of smooth muscle (muscularis mucosa). In the abdominal part, the musclaris mucosa is lined by columnar epithelium similar - the squamo-columnar junction
- Submucosa containing the mucous secreting tubular glands (seromucous glands) and also contains blood vessels, lymphatics and nerves in abundance.
- Muscularis externa: upper third of oesophagus is striated, skeletal muscle under conscious control for swallowing. The lower two thirds are smooth muscle under autonomic control (peristalsis). The muscularis externa consists of an outer longitudinal and n inenr circular layer, like the rest of the GI tract.
Describe the 2 sphincters of the oesophagus
- The upper oesophageal sphincter, which is a striated muscular (anatomical) sphincter and part of the cricopharyngeus muscle. Normally constricted to prevent air entering the oesophagus.
- The lower oesophageal sphincter, which is a physiological sphincter and made up of the lower 2-3cm of oesophageal smooth muscle. This is the intra-abdominal segment of oesophagus. It acts like a flap valve and with the muscosal rosette formed by folds of gastric mucosa, helps to occlude the lumen of the gastro-oesophageal junction.
What are the 3 phases of swallowing? Describe the first two in detail
Swallowing is in 3 phases: the voluntary phase, where a bolus is moved onto the pharynx, the pharyngeal phase and the oesophageal phase
- The voluntary buccal phase occurs when mouth is closed. The bolus of food is pushed upwards and backwards against the hard palate, pushing it into the pharynx.
- In the pharyngeal phase afferent information from pressure (mechano)receptors in the palate and pharynx reaches the swallowing centre in the brain stem, which then triggers a set of movements, including the tongue being positioned against the hard palate preventing the bolus re-entering the oral cavity, the nasopharynx being closed off by the soft palate in particular the uvula, the larynx is elevated and its opening sealed off by the vocal cords, the epiglottis closing the larynx, inhibition of breathing, closure of the glottis and the opening of the upper oesophageal sphincter. Once the bolus has passed through, the UOS contracts tightly.
What happens in the oesophageal phase of swallowing?
- The muscle of the upper third of the oesophagus is voluntary striated muscle, under the control of somatic nerves.
- The muscle of the lower two thirds is smooth muscle, under the control of the parasympathetic nervous system.
- In the oesophageal phase, a wave of peristalsis sweeps down the oesophagus, propelling the bolus to the stomach in about 9 seconds. This is coordinated by extrinsic nerves from the swallowing centre of the brain. Lower oesopageal sphincter opens.
- The LOS relaxes when the peristaltic wave meets it. It opens, allowing the bolus to pass into the stomach. Precision of tone is given by the vagal excitatory fibers (cholinergic) and the vagal inhibitory fibres (non-adrenergic non cholinergic) which act reciprocally.
- To tighten the LOS, an up-regulation in vagal excitatory fibre stimulation is required, coupled with a down-regulation in vagal inhibitory fibre stimulation.
- Swallowing: important brainstem function. Must be checked, especially after head injury / surgery
Very high risk of aspiration
Absent in brain death
What is Dysphagia and Odynophagia? How may Dysphagia occur?
Dysphagia: the symptom of difficulty of swallowing
Odynophagia: the symptom of pain whilst swallowing
- Dysphagia may result as a consequence of a primary oesophageal disorder for example motility problems of the smooth muscle preventing peristalsis (this is known as achalasia)
- Dysphagia may also result as a secondary consequence of another tissue e.g. obstruction or compression of the oesophagus due to a tumour, mouth cancer, or Gastro-oesopahegal reflux disease (the reflux of acidic gastric content through the lower oesophageal sphincter).
Outline the anatomical relationships and location of the oesophagus
- The oesophagus begins at the inferior border of the cricoid cartilage, where it is continuous with pharynx. Initially it inclines to the left, but is moved medially by the aortic arch at the level of T4
- Inferior to the arch, it inclines to the left and passes through the diaphragm, just left of the median plane
- In the superior mediastinum, it lies anterior to the first four thoracic vertebrae and posterior to the trachea, left main bronchus and left recurrent laryngeal nerve.
- At the level of T5, the oesophagus moves forward and to the left, to descend behind the fibrous pericardium and in front of the descending aorta.
- The oesophagus enters the abdomen through the oesophageal hiatus in the muscular part of the diaphragm, at the level of T10.
Categorize different types of dysphagia based on the underlying pathology
Dysphagia can be split into 2 categories:
Dysphagia for solids:
- Oesophageal dysphagia
- Endoscopy – worried about a blockage or a tumour
Dysphagia for liquids
- Oropharyngeal dysphagia
- Videofluroscopy – you drink a fluid contrast so you can see the liquid going down in a controlled environment (so you can see the swallowing process)
- Most commonly due to a stroke
Describe the anatomical mechanisms that prevent gastro-oesophageal reflux
- The stomach produces strong acids (HCl) and enzymes (pepsin) to aid in the digestion of food. The mucosa of the stomach provides protection from its harmful content but the mucosa of the oesophagus does not have this protection
- The oesophagus is protected by the lower oesophageal sphincter which acts like a one-way valve. This coupled with the angle of His that is formed at the junction of the oesophagus and the stomach, prevents reflux of the stomach’s contents.
- The crus of the diaphragm helps with the sphincteric action.
- Apart from the physiological lower oesophageal sphincter, other factors which help prevent reflux of gastric contents are the abdominal pressure acting on the intra-abdominal part of the oesophagus, the valve-like effect of the oblique angle between the oesophagus and the stomach, the pinch-cock effect of the diaphragm on the lower oesophagus and the plug-like action of the mucosal folds
What are the consequences of free gastro-oesophageal reflux?
Barrett’s Oesophagus:
- abnormal metaplasia from non-keratinised stratified squamous epithelia to columnar epithelium and goblet cells. This is an attempt to better resist the harmful contents of the stomach.
- Strongly associated with adenocarcinoma, a particularly lethal cancer
Gastro-oesophageal Reflux Disease: the reflux of the stomach’s contents into the oesophagus causes several symptoms including a hoarseness, heartburn, dysphagia and chest pain, asthma, cough.
- -Pathogenic mechanisms include the resting LOS tone being low or absent, poor oesophageal peristalsis leads to reduced clearance of acid in the oesophagus, a hiatus hernia can impair the function of LOS and the diaphragm closure mechanism as the pressure gradient between the abdominal and thoracic cavities is diminished, delayed gastric emptying increases the chance of reflux.
