Classification and Clinical Features of Haematological Malignancies Flashcards
(22 cards)
How common are haematological malignancies?
- Prevalence - how many cases are there per 100,000 population?
- Incidence - how many new cases are there per 100,000 population?
- Overall, haematological malignancy accounts for approimately 8-10% of all new cancer diagnoses.
Describe the presentation of acute myeloid leukaemia (AML) and lymphoblastic leukaemia (ALL).
- Fairly non-specific presentation. May have a pancytopaenia and leukaemic cells in the blood.
- Marrow failure:
- Anaemia
- Thrombocytopaenia
- Neutropaenia
- FBC normally raises strong suspicion - blast cells seen.
- Myelodysplasia (MDS) - progressive marrow failure.
- This is a pre-leukaemic syndrome (fairly common).
- A proportion of them evolve to acute leukaemia. First they have marrow failure, they get anaemic and possibly thrombocytopaenic, then a proportion go on to have leukaemia.
- Pancytopaenia and risk of evolution to AML.
What are the treatment principles for AML / ALL?
- Induction chemotherapy to induce remission - 4-6 week inpatient stay.
- Wipe the marrow clear and rely on the stem cells to repopulate the marrow space.
- It is like a flowerbed with weeds. Apply a liberal coating of weed killer and hope that the flowers have a more substantial power to regenerate than the weeds.
- If a patient is 60 or 70 you need a good reason to not attempt this. If they are 80 or above you need a good reason to go ahead with this because it is intensive (good cytogenetics, no multimorbidity etc.).
- Consolidation chemotherapy to impact minimal residual disease (MRD).
- Maintenance chemotherapy and CNS prophylaxis for ALL.
- Stem cell transplant for high risk or relapsed disease.
- Some elderly / frail patients for supportive care alone.
What is the survival rate in AML/ALL patients?
- 75% of paediatric ALL is cured - some with long term toxicities.
- AML depends on age and genetic factors.
Describe the presentation of chronic myeloid leukaemia.
- The cells in this disease seen in the peripheral blood are the mature cells.
- Bone pain from marrow expansion.
- Pain from splenomegaly.
- Chance finding.
- Diagnosis from FBC / marrow including cytogenetics (Philadelphia chromosome) and molecular studies BCR-ABL fusion gene.
What are the treatment principles in CML?
- Treatment options:
- Targeted cancer drugs
- Chemotherapy
- Bone marrow and stem cell transplant

Describe the survival of CML in patients.
- Well-tolerated orally active tyrosine kinase inhibitors.
- Almost all patients have similar mutation - targeted therapy.
- Managing toxicities and monitoring MRD.
- Few patients now evolve to ‘blast crisis’.
- There has been a dramatic improvement in survival in the last generation.

Describe the presentation of myeloma.
-
Plasma cell
- Also, pre-malignant condition of Monoclonal gammopathy of undetermined significance (MGUS).
- Clone of mature B cells producing antibody - IgG/IgA/light chains.
- Crowding out of marrow - anaemia.
- Hypercalcaemia - Ca2+ mobilised from bone by osteoclasts.
- Bone pain and fractures - lytic destruction of bone cortex.
- Bony cortex has had the calcium and the matrix taken out. Punch-hole lesion - roughly round.
- Renal impairment - tubular damage by precipitated light chains.

What are the treatment principles in myeloma?
- Behaves as chronic relapsing disease with treatment-free intervals but very rarely curable.
- Supportive care:
- Managing anaemia - transfusions / EPO.
- Maintaining renal function - fluids / avoid nephrotoxins / treat elevated Ca2+.
- Bone pain - control myeloma / fixation of fractures / bisphosphonates.
- Radiotherapy - for localised bone pain or fractures.
- Chemotherapy - to obtain response / remission and halt organ damage:
- Steroids e.g. dexamethasone
- Cytotoxics e.g. cyclophosphamide
- Immunomodulatory e.g. thalidomide
- Stem cell transplant - used particularly in <70
- Proteasome inhibitors e.g. bortezomib
- Monoclonal antibodies
- Some are used to maximum response and stop, some are ‘maintenance’ or treat till diseases progression.
Describe the survival of myeloma.
- Elderly deaths in frail patients with organ failures.
- Improvement in recent years (chronic relapsing disease) but life-limiting in most patients.

Describe the presentation of chronic lymphocytic leukaemia (CLL) and Non-Hodgkin’s lymphoma (NHL).
- CLL >50% will be a chance finding on a blood count and the remainder slowly evolving lymphadenopathy / splenomegaly +/- anaemia.
- Low grade lymphoma (commonly follicular and marginal zone (NHL) slowly evolving lymphadenopathy / splenomegaly.
- They are often ‘not ill’.
- >20% are extra-nodal presentation, for example:
- GI tract
- Salivary gland
- Skin
What are the treatment principles for CLL and low-grade NHL?
- Slow pace of disease (many years), not curable unless very localised.
- Majority are B cell-derived. Some are T cell derived.
- ‘Watch and wait’ for most CLL and some low grade NHL new patients.
- Treat if symptomatic / bulky disease / organ damage.
- Typically chronic relapsing diseases.
- Steroids e.g. prednisolone.
- Cytotoxics e.g. cyclophosphamide / vincristine.
- Monoclonal antibodies e.g. rituximab +/- for maintenance.
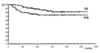
Describe the survival in CLL and low-grade NHL.
- Many elderly patients will die of unrelated causes.
- Some die of progressive disease - drug resistance / organ failure.
- Some transform to more aggressive disease.
- Picture - survival in CLL by age at presentation.

Describe the presentation of high grade NHL.
- Most are diffuse large B cell NHL, Burkitt’s mantle cell.
- Rapidly progressive lymphadenopathy - superficial sites or internal.
- Often unwell with ‘B’ symptoms:
- Weight loss >10% in <6 months
- Heavy sweating
- Fever to 38°C
- 10-20% are extra-nodal presentation.
What are the treatment principles in high grade NHL?
- Chemotherapy e.g. R-CHOP (If fit for intensive and ?curative Rx)
- Rituximab
- Cyclophosphamide
- Adriamycin
- Vincristine
- Prednisolone
- Frail patients:
- Prednisolone +/-
- Oral chemotherapy
- Palliation
- Radiotherapy after limited chemotherapy for localised disease.
- More aggressive chemotherapy or autologous stem cell transplant for relapsed disease.
Describe the survival from high grade NHL.
- Curable disease, but depends on histology / age / frailty.

Describe the presentation of Hodgkin’s disease.
- Painless, progressive lymph node enlargement.
- B cell origin (Reed-Sternberg cell).
- Staging and age / sex / lymphopaenia / anaemia
Summarise the stages of Hodgkin’s disease.

What are the treatment principles in Hodgkin’s disease?
- High cure rate - adjust intensity of treatment to risk factors and initial response to treatment.
- Chemotherapy +/- radiotherapy (for localised, bulky or residual disease).
- PET scanning to show metabolic activity as wellas size / shape.
*

Describe the survival from Hodgkin’s disease.
High cure rate but some long-term toxicities and 2nd malignancies.
Describe the presentation of myeloproliferative disorders / neoplasms.
- Chance finding on blood count. For example:
- High Hb (polycythaemia vera) - can also be secondary to hypoxia or low plasma volume.
- High platelet count (essential thrombocythaemia) - can also be reactive e.g. to inflammatory process.
- Can present with thrombotic or bleeding episodes or splenomegaly.
- Molecular markers e.g. Jak-2 mutation can aid diagnosis.
What are the treatment principles in myoproliferative disorders?
- Normalise blood count to reduce vascular risk - venesection and / or hydroxycarbamide.
- Natural hx includes evolution to myelofibrosis or AML.

