Anatomy, MCP and Histology Deck Flashcards
What components of the cell is labeled by hematoxylin stain?
-heterochromatin, RER, and sulfated GAGs
What components of a cell are labeled by Eosin stain?
cytoplasm, cytoplasmic filaments, and collagen fibers and basment membrane
What type of epithelium is best designed to protect against abrasion?
Stratified squamous epithelium
What two functions of simple squamous epithelium?
active transport via pinocytosis and secretion of biologically active molecules
Define stereocilia
microvilli of the male reproductive tract
Define striated border
microvilli of Intestinal Epithelial cells
Define brush border
is the microvilli of renal proximal tubule
What is hyperplasia mean?
means an increase in cell number
what is hypertrophy?
increase in size
what is dysplasia?
change in organization
what is metaplasia?
transformation to another cell type
Compare cilia vs. microvilli
cilia:
-microtubules in a 9+2 arrangement covered by cell membranes
Microvilli:
-finger like extensions on the apical surface of epithelia cells
Name 2 tissues that have basement membrane
simple cuboidal and simple squamous
simple cuboidal functions
corvering and secretion
simple columnar functions
secretion, absorption, lubrication, and protection
strafitied squamous functions
protection (“wear and tear”), and prevention of water loss
ie. anal canal, mouth, vaginal canal and skin
Stratified cuboidal functions
protection and secretion
what functions of transitional epithelium?
Protection and distensibilty
Stratified Columnar functions
Protection
Dense Regular Loose CT what is it
- more
- loose connective tissue which has more fibers than cells
- forms parallel bundles or sheets
- found in tendons, ligaments, and cornea
Dense irregular CT
- loose CT that there are more fibers than cells
- fibers are interwoven
- found in organ capsules, periosteum, and reticular layer of dermis
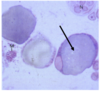
What cell is virtually stained with trypan blue
Macrophages
What cell is identified in the blue? What is the stain used

Macrophages
Trypan blue
The cell that is the most common CT cell
Fibroblasts
This cell is derived from B lymphocytes
Plasma cell
WHat cell has heparin containing granules?
Mast cells
WHat cell can serve as adult stem cell tissue?
Mesenchymal cells
WHat fiber is stained with silver stain
Reticular fibers
What CT fibers would allow stretch and recoil of blood vessels?
Elastic fibers
What CT fiber is composed of collagen type 3?
Reticular fibers
what CT fibers is composed of collagen type 1?
what is collagen type 1 produced by?
what is its function?
collagen fibers
Fibroblasts
Resists stretching
The most abundant fiber type in lymphoid tissues is
Reticular fibers
What CT fibers contains desmosine and Isodesmosine?
Elastic Fibers
Forms the largest diameter in loose CT
collagen fibers
What are three basic components of all types of connective tissue?
Tissue fluid, Ground substance, and Protein fibers
multiocular fat (function, and lipid droplet content)
less lipid droplet than uniocular (smaller in size)
- important for fetus development as it thermally insulates fetus (transfers chemical energy into heat)
- aka known as brown fat.
what is the order of size in the 3 main CT types? (greatest to smallest)
Collagen> Reticular> Elastic
Uniocular fat (function, lipid contact and structure)
- most adipocytes common in adults
- contain large amount of lipid droplets( containing fatty acids and triglycerides)->largest repository in body
- surround many areas and orgrans under the skin with role of thermal insulation filling spaces to properly position organs
- larger than multiocular fat
type II collagen function
resists pressure
What type of loose connective tissue is shown in the picture

Dense Regular
What is shown by 1 and 2?

1- Goblet cell
2- Cilia
WHat is shown by the arrows?

Dome cells as the bladder is stretched
What is shown by the arrows?

-The dome cells of relaxed bladder
What is shown by the arrows?

vascular islands
What cells are shown in the picture (dark purple) and TEM

mast cells (remember have heparin granules which are seen in stain and TEM)
What cell is shown in the picture?
what is this structure’s function?

Plasma cell (remember has clock looking nucleus)
Produce immunoglobulins
What is the cell in the diagram
What is present in nucleus (the dark areas)

Plasma cell
clusters of euchromatin
what cell is shown below?

plasma cells
what cell is present in the picture?

Fibrocyte
what is this an example of in the picture?
What is it stained with?

Reticular fiber
Silver stain
What tissue is bracketed in the picture?

Loose CT Dense Irregular (remember fibers are interwoven)
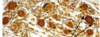
What is shown by the picture?
When there is an H&E stain on adipocyte what happens?

Adipocytes (white fat)
cell stained but with loss of lipid droplet
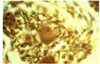
Describe the 2 clues that lets you know this fiber (hint: what is this CT)

1- idaho potato nucleus with prominent nucleolus
2-sample is acid stained
What is shown in the picture?

Fibroblasts
what is shown by the arrow?
what epitheilial cells are present here?
What organ is this tissue of?

small blood vessel
simple cuboidal epithelium
Thyroid
What is shown by the blue arrow?
What is shown by the black arrow?

shows the thickness of the epidermal layer (stratified epithelium)
-boundary line between epidermis and dermis (contains basement membrane)
What is a herd immunity?
This is when enough individuals in a population are vaccinated such that the spread of infection is slowed or halted
What is active immunization?
what is some advantages?
this when you use antigen to induce an immune response to a pathogen
advantage: is longterm
what is passive immunization? what is a disadvantage?
when you use immune serum to provide immediate resistance to an infection.
Disadvantage: is temporary
what is the difference between DPT and Dtap?
Which would be better to use? why?
DPT used killed pertussis and Dtap was a toxoid with alum salts (adjuvant) vaccine
Dtap because it has less adverse effects than DPT (was nasty vaccine with severe effects)
why has there been an increase in autism with increase vaccinations? is it due to vaccines?
no its been due to changes in the DSM including more behaviors in the category of Autism
Live attentuated viruses are contraindicted for 3 groups people which are
1) Pregnant woman
2) Immunocompromised (ie. Cell-mediated or Humoral Immunodeficiency)
3) Children under the age 1
What is cartilage made from? and where do they embed themselves
chrondrocytes and are embedded in matrix within lacunae
What are three types of cartilage?
hyaline cartilage, elastic cartilage, and fibrocartilage
Hyaline cartilage (where is it found?)
- the most common cartilage
- found in the vental ends of ribs, tracheal rings, larynx, bronchi, articular surfaces of bones (bone ends, epiphyseal plates, and nose)
Elastic cartilage (where is it found?)
Elastic cartilage is found in areas where flexibility is needed
- pinna of the ear,
- epiglottis,
- several laryngeal cartilages (vocal cords)
and eustachian tubes.
What collagen fiber is most common in hyaline cartilage?
type 2 collagen (remember it resists pressure)
chrondrocytes (what are they and what do they contain?)
protein-secreting cells which are embedded in matrix
- contain diffuse chromatin and alot RER and mitochondria
- contained well developed golgi apparatus
isogenous groups in an active chondrocyte are a result of
chondrocyte division (of up to eight cells) as it is isolated by matrix
Why is the cytoplasm of an active chondrocyte basophillic?
contains a higher concentration of sulfated GAGs in the capsular matrix (than the interritorial matirix)
Why does cartilage have a poor potential for repair after injury?
Cartilage is avascular tissue (except for in young children)
Fibrocartilage (where is it found?)
Intervertebral discs and Pubic symphysis
What are the principal components of ECM of cartilage?
Chondrocytes
Collagen
hyaluronic acid
Proteoglycans
glycoproteins
water
Fibrocartilage contains most which collagen type?
contains mostly collagen type 1 (remember type 1 forms fibrils)
How does Fibrocartilage differ from the other types of cartilage?
- contains no perichondrium
- basically a combination of hyaline and dense regular connective tissue
- chrondrocytes are similar in shape to other types of cartilage
During chondrogenesis, you have two types of growth which are
interstitial growth and appositional growth
appositional growth is
- growth accomplished by the addition of new layers to those previously formed
- cartilage growth from new chondroblasts which are in the perichondrium. (add a new layer of ECM precursor cells and components and then those precursors cells make new chondroblasts which make new cartilage (cycle repeats)
chrondrogenesis occurs in the pathway of
mesenchymal cell -> Condensed chondroblast-> ECM secretion -> isogenous groups
can interstitial growth happen in bone? what happens instead? How about cartilage?
No only in cartilage it happens. Only appositional growth occurs in bone
cartilage can undergo, both interstitial and appositional growth
Interstitial growth is
-growth from the pre-existing chondroblasts
growth occurs in the process of endochondral ossification
when an osteoblast differentiates it produces
new bone matrix and an osteocyte
What are the principal components of Bone
- calcified ECM (bone matrix)
- in the bone matrix three types of cells (osteoclasts, osteoblasts, and osteocytes)
Once an osteocyte is formed it is present in its very own secretions of matrix and are isolated in
Lacunae
In bone osteocytes are able to communicate with eachother via what
gap junctions called canalculi
When osteoblasts are not active they become
osteoprogenitor cells
osteoblasts (what is its function, shape, and morphology)
- responsible for making new bone matrix (osteoid)
- are cuboidal or columnar
- have basophillic cytoplasm
osteoclasts (morphology and function)
- multinucleated large cells are involved in the breakdown of bone matrix
- secrete lysosomes, and acids to bone matrix, causing bone matrix resorption
osteoprogenitor cells ( morphology and function)
mesenchymal stem cells which have the potential to become osteoblasts.
-less active osteoblasts become these cells
4 bone types
woven bone, lamellar bone, compact bone, spongy bone (aka cancellous bone)
what is this tissue from?

Larynx
what cells are represented in this figure

Mast cells
woven bone
nonlamellar and is made in random mix of collagen 1 fibers
-is first to appear in embryonic development and fracture repair
lamallar bone
is spongy bone (cancellous bone) and compact bone
what covers or lines all internal surfaces of bone?
endosteum
What cells are represented in the figure?
how do you know?

Reticular cells
the idaho potato nucleus with prominent nucleolous
What are represented by the arrows?

vascular islands
WHAT IS represented by the two arrows

Blood vessels
What is represented by the arrow?
adipocyte (lipid droplet is lost when staining)
WHat is represented by the top arrow?
WHat is represented by the bottom arrow? where would you find it?

uniocular fat ( white fat)- underneath the skin and around organs to properly place them.
multiocular fat (brown fat) -fetus
what cells is represented by the picture

fibrocytes
what is represented by the arrow?

Dense regular connective tissue
what type of cartilage am I looking at?

Fibrocartilage
what is represented by the arrow?

Tendon
what type of cell is this?
how do you know?

adipocyte (multiocular fat) aka brown fat
has many capillaries
What is represented by the arrow

osteoblasts
what is represented by the arrow
how do you know?

osteoclasts
multinucleated cell
what is type of cartilage is represented here?
bonus: what is the tissue on the left of the picture?

fibrocartilage
intervertebral ligament
what is tissue is represented here?
what are pointed by the arrows?

fibrocartilage
chondrocytes
what is the big structure on the left?
What it the smaller picture on the right?
what is the structure on the bottom

that is the baby tooth
permanent tooth
alveolar proceses
what type of bone is represented here?
what is it lined with?
what are the red dots?
what are the red dots connected by?
what is the yellow stuff?

cancellous bone (spongy bone)
endosteum
osteocytes
gap junctions processes called canalculi
marrow cavity
what part of the bone are we looking at?
what is represented by the arrow in the bottom?
What is represented by the pointers above it? what is lined with
what is the yellow?

compact bone
periosteum
haversian canal (osteon)
lined with endosteum
marrow cavity
what is represented by the yellow?
What is represented by the bone that penetrates the yellow region?
What is represented by the darker encircling bone?
what covers the bone in this figure

marrow cavity
spongy bone
compact bone
periosteum and then connective tissue(outermost)
What tissue am I looking at?
What is represented by the arrows?

Elastic cartilage
elastic fibers
what organ am I looking at?
what is it primarily composed of (cartilage)

the pinna of the ear
elastic cartilage
What anatomy is represented by the top dashed line?
What about the second dashed line?

1) anatomical neck
2) Surgical Neck
Fractures to the humerus happen where the most?
What nerves and arteries would most likely be damaged?
What disease would this put you at risk in?
Surgical Neck
axillary nerve and posthumeral circumflex artery
avascular necrosis (anatomtical neck
What arteries or nerves would be at risk of being damaged if humeral shaft fracture
Radial artery and nerve
Fracture of the medial epicondyle would result in damage in what nerve?
ulnar nerve
Fracture of the lateral epicondlye would result in damage in what?
Radial artery and Radial nerve
Tell me the anatomy of the scapula from 1-10 (except 3)

- Acromion Process
- suprascapular notch
3.
- superior border
- medial border (vertebral border)
- Inferior border
- subscapularis fossa
- Lateral (axillary border)
- Glenoid cavity
- coracoid process
- supraspinous fossa
- Scapular spine
- Infraspinous fossa
- Lateral border (axillary border)
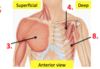
Name A-J of the shoulder (except D)

A. Acromioclavicular Ligament (aka AC joint)
B. Acromion Process
C. coracoaromial ligament
E. tendon of the Biceps Brachii
F. Lesser Tubercle
G. Glenohumeral joint
H. Coracoid process
I. Coracoclavicular ligament
J. Clavicle
K. Greater Tubercle
Name the anatomy of muscles 1 through 7 (except 3 and 4)

- Trapezius
- Latissmus Dorsi
- Levator Scapulae
- Rhomboid Minor
- Rhomboid Major
Name the anatomy of 3,4,8
- Pectoralis Major
- Pectoralis Minor
- Serratus Anterior
What is the action of the levator scapulae?
Innervation?
to elevate the scapula
dorsal scapular nerve
What is the trapezius action?
Innervation?
Upper fibers : Elevates the scapula
Middle fibers: Retract the scapula
Lower fibers: Depress the scapula and lowers the shoulder
Spinal accessory nerve
What is the action of the latissmus dorsi?
innervation?
adducts, extends, and medially rotates the arms
Thoracodorsal nerve
What is the action of the pectoralis major?
innervation?
clavicular fibers: flexes the humerus
sternal fibers: extend the humerus
all fibers: adducts and medially rotates humerus
medial and lateral pectoral nerves
What is the Innervation pectoralis minor?
Medial pectoral nerves
What are the actions of the Rhomboid major and minor muscles together?
Innervation?
retraction of the scapula
Elevation of the scapula
Downward rotation of scapula
(Think R.E.D)
Dorsal scapular nerve
What is the innervation of Serratus Anterior?
Long Thoracic Nerve
What are the muscles for 1-6?

1) Supraspinatus
2) Infraspinatus
4) Teres Minor
5) Teres Major
6) Deltoid
The levator scapulae, rhomboid major and minor are all innervated by the
dorsal scapular nerve
What is the innervation of Teres Minor?
Axillary Nerve
What is the action of the subscapularis?
innervation?
adducting and medial rotation of the arm
upper and lower subscapular nerves
What is the rotation cuff muscles?
S.I.T.S
Supraspinatus
Infraspinatus
Teres Minor
Subscapularis
What is the Innervation of Teres Major?
Dorsal scapular nerve
Deltoid Muscle action is
innervation?
anterior fibers:
flexion of the arm
posterior fibers:
extension of arm
all fibers:
abduction of arm
axillary nerve
What is sarcoplasm
cytoplasm of the muscle fiber
What is sarcolemma?
muscle fiber (specialized) plasma membrane
What is Sacroplasmic Reticulum?
muscle fiber specialized version of smooth endoplasmic reticulum (contains Calcium stores)
Is a sarcoplasm eosinophillic or basophillic? why?
strongly eosinophillic (due to its cytoplasmic filaments)
What is an excitable cell?
cells that generate action potentials
Which muscle types are mononuclear? Which are multi-nuclear?
1) Smooth Muscle
2) skeletal and cardiac muscle
How does the position of nuclei differ between muscle fiber types?
- Smooth and cardiac muscle nuclei are centrally placed
- Skeletal muscle nuclei are peripheral
1) WHy do some muscle fibers appear striated when viewed by light microscopy?
2) which are striated?
1) due to lateral alignment of sacromeres (contractile units)
2) Skeletal and cardiac muscle
What are dense bodies?
-electron dense bodies that anchor the thin filaments
- they are in smooth muscle and replace z discs found in the other muscle types.
- at the sacrolemma they form cell-cell and cell-ECM attachments
What muscle types have cell-cell junctions between muscle fibers? what roles do they play?
Smooth muscle and Cardiac muscle
-play a role in propagating the action potential to neighboring cells causing more synchronized contraction
Which muscle type appears most similar to its mesenchymal cell precursor? why?
Smooth muscle
it is least differentiated from its mesenchymal precursor cell (therefore looks most like it)
*Note it also makes sense why they are able to replicate
For skeletal muscles and cardiac muscles what cell attachment structures are present on the lateral surfaces of fibers? what are their function?
Costameres
- cell-ECM junctions on the lateral surfaces of some muscle fibers whose function is to stabilize the plasma membrance during contraction
What attachments are at the fiber ends of cardiac and skeletal muscle?
intercalated discs and myotendinous junctions
Which muscle types regenerate? how do their mechanisms of regeneration differ?
smooth muscle and skeletal muscle
smooth muscle due to it not being as differentiated from mesenchymal precursor can just replicate so damage is replaced
For skeletal muscle are able to regenerate by satellite cells
WHat is the name to the outer layer of dense irregular connective tissue of skeletal muscle?
Epimysium
What surrounds skeletal muscle fascicles?
WHat separates the fibers in the fasicicle?
Perimysium
Endomysium
WHat muscle types contract rapidly?
What internal membrane structures in their muscle fibers assist? How do they assist?
Cardiac and skeletal muscle
SER, T-tubules
They assist by forming a muscle triad which is one tubule plus 2 SER cisternae
via action potential they allow Ca2+ release which leads to contraction.
Which muscle type is associated with pathologies involving over-proliferation of muscle fibers.
Name one of those pathologies.
- smooth muscles
- atherosclerosis
What is a purkinje fiber?
is a cardiac muscle fibers specialized to rapidly conduct action potentials
-have a large diameter and are located in the inner walls of the ventricles
WHat is a muscle spindle?
It is a specialized muscle fiber that is a sensory organ for stretch
Which muscle types are under voluntary control?
only Skeletal muscle
The Supraspinatus and Infraspinatus are innervated by the
suprascapular nerve
What is identified by this structure?

Pacnian Corpuscle
WHat is identified by the arrow?

Meissners Corpuscle
What is represented by the picture?
what would be an example of this?

Sensory ganglion
Dorsal Root Ganglion
WHat is represented by the arrow?

Myleinated axons
What neuron is represented by the picture?
How would you know?
Autonomic Neurons
nucleus is usually off center (acentric) and has many processes and alot of satellite cells
What is represented by the picture?
autonomic ganglion (multi-polar neuron)
What is represented by the three layers? (top to bottom)

- cross section of smooth muscle
- Auerbach’s Plexus
- Longtudinal section of smooth muscle
what is represented by the arrow?
what is the layer beneath the arrow?
WHat layer is outside the arrow?

perineurium
Endoneurium
Epineurium
what is represented by the circle?

Node of Ranvier
What is represented by the circled structure?

Schmidt-Lanterman clefts
How do you distinguish myleinated form unmyleinated nerve fibers in an H&E stained tissue section?
TEM?
You can see the schmidt-lanterman clefts, and presence of node of ranvier in myleinated axons.
Unmyleinated neurons usually have thin schwann cell fold which normally contain multiple thin unmyelinated axons.
What is the node of Ranvier?
this is the place where the the schwann cell is adjacent to another schwann cell.
The perineurium is the most (blank) of the connective tissue components of a peripheral nerve
prominent and visible
What fixative will preserve mylein for light microscopy?
What type of neuron has its cell body in a dorsal root ganglion?
sensory neuron
Which type of ganglion contains numerous unmyleinated fibers?
sensory ganglion
What type of receptors is located in the post-synaptic membrane of a neuromuscular junction?
acetylcholine receptors
What morphological features distinguish a pacnian from a meissner’s corpuscle?
- both are encapsulated endings
- pacnian (has concentric layers of flattened schwann cells) looks like an onion
- meissners looks like its stacked like coins
What are the functions of sensory free nerve endings in the skin?
List two functions of a muscle spindle
What is the action of the tricep brachii?
Innervation?
extension of the forearm
Radial nerve
What is the action of the anconeus?
Innervation?
extension of forearm (synergist to the tricep brachii)
Radial Nerve
What are the definitions of primary and secondary lymphoid organs? (include examples)
Where does the recombination of B cell and T cell receptor genes take place?
Primary lymphoid organs (thymus and bone marrow)are the main producers of your lymphocytes. Secondary lymphoid are the areas where the lymphocytes mature (ie. spleen, lymph node)
Recombination of Bcell receptor genes happens in the bone marrow
Recombination of the T cell receptor happens in the thymus
What are the functions of reticular cells?
The functions of the reticular cells are to produce reticular fibers that provide :
Structural support, guide to cell migration, and filtration
What is the embryological origin of the thymus?
originates from the third pair of pharyngeal pouches(endoderm), which forms embryological epithelium
(usually fully formed at birth and starts to shrink after puberty)
What are the differences between fetal and adult thymus?
fetal thymus is larger
adult thymus is smaller due to involution
Which steps of the T cell maturation occur in the cortex and the medulla of the thymus?
Stage 1) Positive selection happens in the cortex
then
Stage 2) Negative Selection which happens in the medulla
How are the epithelial reticular cells (thymic epithelial cells) different from the reticular cells?
*Give me at least 3 differences
reticular cells make reticular fibers needed for guiding cell migration, and filtration and structural support and Epithelial reticular cells are APC cells that produce elements (cytokines, MHC self-pepitides, etc.)
that guide T cell maturation.
What are the differences between epithelial reticular cells in the cortex and the medulla of the thymus?
Epithelial reticular cells of the cortex present self-MHc for the T cells to bind to (positive selection)
Epithelial cells of the medulla present self peptides (negative selection)
What cell types are present in lymph node?
In what part of the node are they located?
Reticular cells,
Antigen presenting cells (Macrophages, Dendritic Cells),
Follicular dendritic cells (FDCs)
Plasma Cells
Others (Neutrophils)
List the structures in the lymph node in the order of flow of the lymph.
Connective tissue capsule->Trabeculae->Cortex->Deep cortex-> medulla
What are the high endothelial venules? Where in the node are they located ? What is their function?
Hev are endothelial cells that act as surface receptors to attract lymphocytes
- composed of cuboidal epithelium
- functions to allow for lymphocytes to pass through capillary walls (diapediesis)
What are the differences between reticular cells, dendritic cells and follicular dendritic cells?
reticular cells are mesenchymal in origin and make reticular fibers for structural support, guiding cell migration, and filtration
Dendritic cells are antigen presenting cells which present MHC and arrive with the lymph to the lymph node
Follicular Dendritic cells are not related to DCs (are not APCs) but contain complement Fc receptors so they can aggregate Ags and attract and organize lymphocytes.
How do the tonsils differ from the lymph node?
Tonsils are located in the posterior oral cavity and nasopharynx and are associated with surface epithelium (localized there
Lymph Nodes are bean shaped organs abundant in axillae, groin, thorax, abdomen.
What are the major functions of the lymph nodes and the spleen?
Functions of the lymph nodes:
- To filter lymph before it enters the blood stream
- Generates T lymphocytes and plasma cells which produce antibodies
Functions of the spleen:
-filter from from blood:
antigens, red blood cells, and produce antibodies and activated lymphocytes
also store blood
List the blood vessels in the order of flow of blood through the spleen.
Trabecular arteries-> Central arterioles-> Penicillar arter-> sinusoid-> Red pulp veins -> Trabecular veins
What are the components of the white pulp? how do they differ in their B and T cell compositions?
components of white pulp:
Plasma Cells
Primarily T cells
macrophages
Dendritic cells
Compare the open versus closed circulations in the red pulp of the spleen?
Closed circulation: (capillaries to S-irculation)
capillaries connect to sinusoids
Open circulation: (capillaries to chords)
capillaries open into chords
What are the stave cells? What role do they play in the RBC removal?
Stave cells are elongated endothelial cells that line the sinusoids
they are oriented parallel to blood flow
they function to filter damaged, and old, red blood cells and allow healthy red blood cells to enter circulation
What is type of tissue is this (its subtype)

Cardiac Muscle
-large amount of mitochondria and the lack of parallel alignment of sacromeres (appear more branched)
What type of tissue is this? how do you know
reticular cell secreting reticular fiber (on the left)
fibroblast secreting reticular fibers (on the right)
What type of tissue is this TEM?

What are the three phases of Chronic Mylegenous Leukemia? Tell me what happens in each one?
C.A.B
Chronic Phase (2-5 years)
- often asymptomatic
- get vague symptoms due to splenomagly
- really high white blood cell count
Accelerated Phase
- Beginning of clonal evolution
- Impairment of neutrophil differentiation
Blast phase (acute form of disease)
-rapid dividing of abnormal cells (high level of blasts)
For all patients who have CML it due to (what mutations)
-translocation in chromosome (usually but not always the t,9;22) causing BCR-ABL1 fusion gene.
How do you diagnose CML?
Blood work looking for BCR-ABL1 gene (ie. FISH and PCR)
What are the three type of responses monitored during treatment? What do each entail? Which ones are better predictions of treatment outcomes?
Hematologic response- monitors normalization of wbc cells
Cytogenetic response- monitors the decrease of ph+ cells (cells with philadelphia chromosome)
Molecular response- monitors decrease in BCR-ABL1 transcripts
-Early or complete Cytogenetic response or early molecular response predict better outcomes
WHat is the biggest factor when it comes to prognosis outcome of CML?
Phase of the diagnosis
- pts in the chronic phase have good response to treatment
- pts in the blast/accelerated phase usually have a poor responses to treatment
WHat did the Marin et al. study show?
-Showed that BCR-ABL1 transcript after 3months treatment of dasatinib predicted the best long term outcomes.
What is BCR-ABL1 gene? What does this gene lead to in the bone marrow?
- its a fusion with a protooncogene (ABL 1 kinase) at the BCR’s N-terminal coiled-coiled domain, creating a monster fusion that has constitiutive kinase activity (it doesnt stop)
leading to :
Increased cell proliferation
inhibition of apoptosis
decreased cell adhesion ot bone marrow stroma
During Chronic to Blast phase progression in CML you have
- Continuous expression of BCR-ABL1
- Clonal Evolution
- Arrest of differentiation by increased Mushashi2 and decreased Numb expression (associated with advancing of disease and death)
- Inactivation of tumor suppressors
- Genomic Instability due to ROS and jacked up regulation of DNA repair pathways
Treatment of CML
- TKIs (Imatinib, dasatinib, and nilotinib)
- Responds best in the chronic phase (up to 80% effectiveness)
with the effectiveness of TKI’s there can be resistance such as primary and secondary resistance. What are each of them
Primary resistance is when you have failure to reach drug target level response due to (Your fault basicallY):
Patient compliance
variation in drug absorption and metabolism
variation in import or export in cancer cells
Secondary resistance is when you have a good initial response followed by a loss of response due to
- new mutations in the BCR-ABL domain
- BCR-ABL1 gene amplification
- clonal evolutiuon
How do you treat CML resistant to TKI’s? What have they currently been trying to use for resistant tKIs in trials? Why was it stopped?
- crank up the Imatinib dose (some can’t handle increased dose)
- Alternate TKI (but doesnt work against T315I mutant)
- Allogenic Stem Cell Transplant (last resort)
They did a trial study with Pontanib and it showed to have a response in all pts. but the best in chronic phase. Trial was discontinued because of the serious arterial thrombotic events
WHat is DMD? (dystrophin muscular dystrophy)
-DMD is a X-linked recessive disease caused by the absence of dystrophin protein.
(due to mutation [Non-sense mutation] that leads to out of frame reading and hence no protein is made.
-Dystrophin protein is an anchoring protein (connecting actin filaments to ECM through forming complex with sarcolemma) needed to stabilize muscle cell sarcolemma to ECM during contraction.
How does BMD differ from DMD?
in BMD you have a mutation (usually in the rod domain maintaining the reading frame) but you still maintain the wild-type, just smaller protein is made, but its functional.
How do you diagnose DMD/BMD?
First check there serum creatine kinase levels
then do molecular testing to look for the presence of duplications or deletions of the dystrophin gene
What is the treatment status for DMD?
-currently no cure, just treat the symptoms such as
physical theraphy for walking issues
- treating cardiomyopathy
- respiratory care (ventilation)
- surgical correction of scoliosis
- glucocorticoids to slow progression down of disease
What is the use of Exon skipping? (what the goal?)
-using this technique to aim to convert the DMD phenotype to a BMD phenotype by skipping exons to restore reading frame using different oligos (depending on the patient’s mutation)
In the Goeman study: (Results and challenges)
Results:
showed using exon skipping of exon 51 via anti-sense oligosaccharide, did produce the dystrophin protein expression at a reduced size.
Pts improved walking distance in 6 mins
Challenges:
- Rapid turnover of oligos
- hardest to penetrate heart muscle cells
- Large number of mutations would need large number of oligos
What about using utrophin as a treatment? (advantages and challenges)
- utrophin is already made in the body but is localized in myotendinous junctions
- minimal adverse effects such as immune because because utrophin is already made in the body.
- research in mice has shown that utrophin levels have improved dystophy pathology with no toxicity.
challenges;
- expression levels so low in body to produce clinical effect
- low bioavailability in humans
- safety timeline unknown
