03-19 PATH of Cirrhosis Flashcards
At the end of this lecture, the learner should be able to: —Describe the histological progression of liver injury leading to cirrhosis —Describe and be able to recognize the histological features of cirrhosis —List the different forms of liver injury and etiologies that can progress to cirrhosis —List and describe (clinicopathologically) the different types of benign and malignant neoplasms that are primary to the liver —Discuss the rising incidence of hepatocellular carcinoma (17 cards)
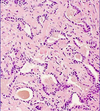
OBJECTIVE: Describe the histological progression of liver injury leading to cirrhosis
- start w/ localized, portal fibrosis
- periportal fibrosis
- bridging fibrosis
- cirrhosis
See slide 19 for bigger version of this image.

OBJECTIVE: Describe and be able to recognize the histological features of cirrhosis

Damage + Regeneration + fibrosis lead eventually to cirrhosis
- causes bridging fibrosis → fibrous septate nodules in liver
- <3mm micronodules
- >3mm macronodules
- end-stage fibrosis is generally irreversible
- hard establish an etiologic dx on morphologic grounds alone once liver is cirrhotic

OBJECTIVE: List the different forms of liver injury and etiologies that can progress to cirrhosis
Forms of Liver Injury
- Intracellular toxic accumulations (iron, fatty acids, acetominophen)
- Inflammation
- Ischemia
Etiologies that can progress to cirrhosis
- Viral hepatitis
- Non-Alcoholic steatohepatitis
- Alcoholic liver disease
- Biliary diseases
- Primary hemochromatosis
- Wilson disease
- α1-antitrypsin deficiency
OBJECTIVE: Discuss the rising incidence of hepatocellular carcinoma
Byproduct of Hep C epidemic
- appx 4 million ppl in U.S. infected
- significant shift of HCC to younger (i.e. 40-60 y/o) age group
What are the three patterns of liver inflammation?
- Which is seen here?

- Portal
- Interface
-
Lobular (parenchymal)
- This here is lobular inflammation, y’all.

Which cell here is gon go crazy and cause collagen deposition → fibrosis ~→ cirrhosis?
- What cytokine encourages it?

activated and proliferating stellate cells → excessive collagen deposition → fibrosis
-
TGF-β which is also the cytokine that (along w/ IL-6) encourages fibroblasts to cause fibrosis in scleroderma
*

What’s up w/ this liver?

Brown color ∆ due to hemochromatosis
—See histo § stained for iron here

This is a liver stained w/ PAS + diastase stain.
- Dx?

Alpha-1-antitrypsin Deficiency

What are the effects of hyperestrogenism seen w/ liver failure?
- palmar erythema
- spider angiomata
- hypogonadism and gynecomastia in ♂
What are the benign and malignant primary liver tumors?

Hepatocellular adenoma (gross sample here)
- Benign or malig?
- Presents in whom?
- Etiology(ies)
- S/Sx
- Dx, including histo?
- Tx?

Benign, 1° liver tumor
Presents in
- Female predominance, 3rd -4th decade
Etios
- Often assoc w/ OCP steroids (duration, potency, type related)
- Androgenic steroids
- Mutated transcription factors HNF1α(50%) and β-catenin(15%)
- Multiple hepatic adenomas (adenomatosis) associated with maturity-onset diabetes of the young type 3 (MODY3) (HNF1α inactivation)
S/Sx
- usually single RUQ mass, pain, hemorrhage/rupture
Dx
- CT
- hepatic angiography
- radionucleide scanning
- biopsy [pic here]: Single-cell plates of nl-looking hepatocytes
- Absence of bile ducts and portal tracts
- may see hemorrhage
Tx
- resect, if > 5 cm
- If < 5cm, just remove OCPs and watch

Focal Nodular Hyperplasia (gross sample here)
- Benign or malig?
- Presents in whom?
- Etiology(ies)
- S/Sx
- Histo

Benign 1° Liver Tumor
Presents in
- All ages; 2♂ : 1♀
Etiologies
- Most likely secondary to vascular abnormalities
S/Sx
- usu asx
- sometimes bleeds
Histo (trichrome image here, H&E on reverse)
- Multiple fibrous septae, w/ typical central star-shaped scar,
- could be confused cirrhosis
- Bile ductular proliferation

Hepatoblastoma (gross sample here)
- Benign or malig?
- Presents in whom?
- S/Sx
- Histo
- Dx
- Tx
- Prognosis

Malignant 1° Tumor of Liver
Presents in
- Usu < 5 y/o kids; 2♂ : 1♀
- Associated congenital anomalies:
- Beckwith-Wiedemann and Down syndromes
- familial adenomatous polyposis
- nephroblastoma.
S/Sx
- Rapidly enlarging upper abdominal mass (diaper doesn’t fit)
- Fever, vomiting, diarrhea, and jaundice are less common
- Virilization & precocious puberty - production of HCG
Histo
- Different histolo subtypes:
- Fetal
- cholangioblastic (on reverse)
- mixed types (here)
Dx
- Elevated AFP
Tx
- Surgery
- Chemo
Prognosis
- Related to tumor stage, unrelated to histologic subtype
5-year survival: 80%

Hepatocellular Carcinoma
- Benign or malig?
- Presents in whom?
- Etiology
- S/Sx
- Histo
- Dx
- Tx
- Prognosis

Hepatocellular Carcinoma
- Benign or malig? MALIG
-
Presents in whom? ♂ >> ♀
- 90% of all primary cancers of the liver
- 3rd most common cause of cancer death worldwide
-
Etiology:
- 80% HBV- or HCV-related
- GLOBAL NORTH: HCV, NASH, EtOH
- GLOBAL SOUTH: HBV, Aflatoxin (grain contaminant)
- Rarely: Metabolic diseases (e.g. glycogen storage dz)
- S/Sx:
- Histo:
- Four subtypes
- solid: hard to distinguish from nl liver
- trabecular: seen here
- acinar: seen on reveres
- mixed
- Also can make four products (see slide 48)
- Mallory hyalin bodies (exact same as EtOH)
- Bile
- A1AT
- cytoplasmic pale bodies: lightly eosinophilic cytoplasmic inclusions (resemble ground glass of hepB, but actually contain fibrinogen)
- Dx:
- Tx:
- Prognosis: Poor

Fibrolamellar Hepatocellular Carcinoma
- Benign or malig?
- Presents in whom?
- Etiology
- Histo
- Prognosis

- Benign
-
Presents in whom?
- younger: 20-40 y/o; ♀ = ♂
-
Etiology
- No association with chronic liver disease
-
Histo: Tumor lobules are separated by wide fibrous bands.
- oncocytic appearance is due to ↑ in # of mitochondria
-
Prognosis
- •Prognosis is more favorable (overall cure rate 50%

What are the benign biliary tumors?
- Which is seen here?
biliary hamartoma (on reverse)
bile duct adenoma (seen here)

What is the malignant bile duct tumor?
- Occurs in
- Histo
- Etiologies
- S/Sx

Cholangiocarcinoma: adenocarcinoma of the bile duct epithelium
OCCURS IN
- Mostly in pts > 60 y/o
HISTO
Clinical and pathologic features depends on the site of origin :
- Small intrahepatic bile ducts – intrahepatic cholangiocarcinoma
- Major intrahepatic bile ducts – hilar cholangiocarcinoma
- Large extrahepatic ducts – i.e. cholangiocarcinoma of the common bile duct
Image here: Mucicarmine stain highlighting mucin in epithelial cells. Presence of mucin is a feature of adenocarcinoma
Image on reverse: Duct-like structures lined by cuboidal epithelium are invested in desmoplastic stroma (new dense stroma induced by tumor)
ETIOLOGIES
- No relation to cirrhosis
- primary sclerosing cholangitis,
- liver flukes (Clonorchis sinensis, Opisthorchis viverrini)
- hepatolithiasis,
- fibrocystic liver disease,
- Thorotrast (radiology dye used in the old days)
S/SX
- Prominent desmoplastic reaction–Irritates surrounding tissue → fibrosis (hard as potato)
- Normal AFP vs. HCC
- ↑ CEA, CA19.9 (serum)

