Trauma - Upper Extremity (Complete) Flashcards
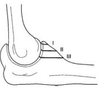
Components of the MCL of the elbow
- Anterior bundle
- Most important for stability (resists valgus)
- Inserts on sublime tubercle (anteromedial facet of coronoid)
- Posterior bundle
- Transverse bundle

Components of the LCL of the elbow
- Lateral ulnar collateral ligament
* Inserts on the supinator crest - Radial collateral ligament
* Inserts on the annular ligament - Annular ligament
* Inserts on the supinator crest - Accessory lateral collateral ligament
* Inserts on the supinator crest

Components of the cubital tunnel
- Roof
- Formed by FCU fascia and Osborne’s ligament
- Travels from the medial epicondyle to the olecranon
- Floor
* Formed by posterior and transverse bands of MCL and elbow joint capsule - Walls
* Formed by medial epicondyle and olecranon

What is/are the classifications for radial head fracture?
[JBJS REVIEWS 2017;5(12):e3]
- Mason
- Type I - Fissure or marginal fractures without displacement
- Type II - Marginal sector fractures with displacement
- Type III - Comminuted fractures involving the whole head of the radius
- Broberg and Morrey
- Type I - displaced <2mm
- Type II - displaced ≥2mm and involving >30% of the radial head
- Type III - comminuted fracture of the radial head
- Type IV - elbow dislocation complicated by any of the above fractures
- Hotchkiss
- Type I - nondisplaced or displaced <2mm without true mechanical block to motion
- Type II - displaced ≥2mm
- Possible mechanical block
- No comminution (ie. amenable to ORIF)
- Type III - severely comminuted and not reconstructible based on radiographic or intraoperative evidence

What injuries are associated with radial head fracture?
- Rupture of MCL
- Capitellum fracture
- Elbow dislocation
- Terrible triad
- Monteggia fracture
- Essex-Lopresti lesions and variants
* AKA Acute radioulnar longitudinal instability - DRUJ injuries
- Carpal injuries
What is the radial head safe zone?
- Nonarticular area of the radial head located posterolateral
- 90-110o arc inline with the radial styloid and lister’s tubercle
- Identified intraoperatively as area of thin cartilage relative to articular portion

What is the treatment of radial head fractures based on fracture displacement and size?
[JBJS REVIEWS 2017;5(12):e3]
Determine the nature of the fracture based on size and displacement
- Undisplaced/minimally displaced fracture (displacement <2mm) OR Displaced and small area of fracture (displacement >2mm and size <33%)
- If no block to motion = treat with early motion
- If block to motion = treat with ORIF (consider fragment excision)
- Displaced and large area of fracture (displacement >2mm and size >33%)
- If reconstructible = treat with ORIF
- Consider radial head arthroplasty
- If not reconstructible = treat with radial head arthroplasty
- If reconstructible = treat with ORIF
What are the contraindications to radial head excision?
- Essex-lopresti lesion
* Defined as radial head fracture plus disruption of the interosseous membrane and DRUJ - Elbow instability
- MCL deficiency
- Coronoid fracture
When performing radial head excision, what should be tested intraoperatively after excision?
[JBJS. 2002 Nov;84-A(11):1970-6.][Journal of Orthopedics 2018; 15(1): 78]
Longitudinal forearm stability
- Radius pull test
- Longitudinal traction applied to proximal radius with clamp (9.1kg) with wrist xray
- >3mm of proximal radial migration indicates IOM disruption
- Radial axial interosseous load (RAIL) test
- Axial load applied through hand and carpus with elbow at 90 degrees
- >3mm of proximal radial migration indicates IOM disruption
- ≥6mm indicates IOM and DRUJ disruption
How many radial head fragments can be present to consider ORIF?
[Tornetta]
≤3 fragments
- If >3, consider arthroplasty
What fixation options are preferred for radial head ORIF?
- One or two countersunk 2.0- or 2.7-mm AO cortical screws perpendicular to the fracture
- Cannulated, headless, resorbable, variable pitched (ie. Biotrak – Acumed)
- AO 2.0- or 2.7-mm mini-plates along the safe zone if fracture extends into the neck
What approach is used for radial head arthroplasty?
[JBJS 2010;92:250-257]
- EDC split if LUCL intact
- Kocher (ECU/anconeus) if LUCL disrupted
* Pronate forearm to protect PIN- Do not dissect distal to radial tuberosity
* Stay above LUCL (above radial head equator)
- Do not dissect distal to radial tuberosity

What is the Mayo classification of olecranon fractures?
[JAAOS 2013;21:149-160]
- Type I = undisplaced
- Type II = displaced but stable
- Type III = displaced but unstable
***Note: each group is subdivided into noncomminuted (A) or comminuted (B)

What is the Schatzker classification for olecranon fractures?
[JAAOS 2013;21:149-160]
- Type A = simple transverse
- Type B = transverse with central articular surface impaction
- Type C = simple oblique
- Type D = comminuted
- Type E = oblique fractures distal to the mid-sigmoid notch
* ‘Oblique distal’ to the greater sigmoid notch - Type F = combined olecranon and radial head fracture
* Often with MCL tear

Which olecranon fractures have intermediate fragments?
[JAAOS 2013;21:149-160]
- Schatzker B+D
- Mayo IIB and IIIB

What is the recommended fixation construct for olecranon fractures based on Schatzker fracture type?
[JAAOS 2013;21:149-160]
- Type A = tension band wire through posterior approach
* Precontoured plates provide greater compressive force than tension band wire - Type B+D = plating with interfragment screws
- Type C+E = plating
- Type F = plating with intefragment screws, radial head and ligament repair

What is the PUDA angle?
[JAAOS 2013;21:149-160]
PUDA = proximal ulna dorsal angulation
- The average PUDA is 6° measured 5cm distal to the tip of the olecranon
- Increased PUDA associated with decreased terminal elbow extension

How do you use the radiocapitellar ratio (RCR) to measure radial head alignment?
[JAAOS 2013;21:149-160]
On a lateral XR, the RCR measurement is the minimal distance between the axis of the radial head and the center of the capitellum, divided by the diameter of the capitellum
- RCR is a valid measurement to assess radial head translation about the capitellum
- Malalignment is an RCR value outside the normal range of -5% to 13%

What is the angulation of the proximal ulna in the coronal plane?
[JAAOS 2013;21:149-160]
Mean varus angulation of 14°+/-4°
- Measured between the axis of the olecranon and axis of the ulna midshaft
What are important considerations in fixation of comminuted olecranon fractures?
[JAAOS 2013;21:149-160]
- Avoid narrowing the greater sigmoid notch
- Obtain anatomic articular reduction with direct visualization of articular surface
- Rigid fixation
- Fixation of fragments should occur from distal to proximal utilizing interfragment screws when possible
- Intermediate fragments can be stabilized with “home run screws”
- Triceps insertion should be reinforced with Krakow stitch in presence of small or comminuted proximal fragments
- When triceps repaird to bone, should be reattached as dorsally as possible to maximize strength
- 24% strength loss still occurs
***Some bone loss can be accepted in the bare area
- Will fill with fibrous tissue as long as posterior cortex is rigidly fixed
Indications for nonoperative treatment of olecranon fractures?
[Rockwood and Green 8th ed. 2015]
- Undisplaced fracture
- Poor surgical candidate
- Displaced fracture in low-demand elderly patient with multiple comorbidities
What are the surgical options for olecranon fractures?
- Olecranon fragment excision and triceps advancement
- Tension band wiring
- Contoured plate
- Intramedullary screw
What are the indications for olecranon fragment excision and triceps advancement?
[Rockwood and Green 8th ed. 2015]
Elderly patients with osteoporosis and/or comminution, involving less than 75% of the olecranon (some sources <50%)
What is the influence of anterior vs. posterior triceps repair following fragment excision and triceps advancement?
[JOT2011;25:420–424]
- Posterior repair = higher triceps extension strength
- Anterior repair = slightly more stable but not statistically significant
What are indications and contraindications for tension band wiring olecranon fractures?
Indications:
- Isolated transverse fracture (no comminution) proximal to the base of the coronoid
Contraindications:
- Comminuted
- Some oblique fractures
- Fracture distal to the bare area involving coronoid base
What are the indications for plating olecranon fractures?
- Comminution
- Oblique fractures
- Fracture extension to the shaft
What complications can occur with overpenetration of the anterior cortex with K-wire during tension banding of an olecranon fracture?
- Anterior interosseous nerve injury
- Impaired pronation/supination due to mechanical block
What are the components of the coronoid?
[JAAOS 2013;21:149-160] [JBJS REVIEWS 2014;2(1):e3]
- Tip
- Body
* Imparts rotational stability - Anteromedial facet
* Resists varus instability - Anterolateral facet
* Resists posterior forces - Sublime tubercle

What is the Regan and Morrey classification of coronoid fractures?
[J Am Acad Orthop Surg 2008;16:519-529]
Based on the lateral radiographic view
- Type I – avulsion of the tip of the process
- Type II – fragment involving ≤50% of the process
- Type III – fragment involving >50% of the process
- IIIA - WIthout elbow dislocation
- IIIB - With elbow dislocation
What is the O’Driscoll classification of coronoid fractures?
[J Am Acad Orthop Surg 2008;16:519-529]
Based on anatomical location of fracture
- Type I – TIP
- Subtype 1 = ≤2mm of coronoid height
- Subtype 2 = >2mm of coronoid height
- Type II – ANTEROMEDIAL
- Subtype 1 = anteromedial rim
- Subtype 2 = anteromedial + tip
- Subtype 3 = anteromedial rim + sublime tubercle (±tip)
- Type III – BASE
- Subtype 1 = coronoid body and base
- Subtype 2 = transolecranon basal coronoid fractures

What type of coronoid fracture is associated with varus posteromedial rotary instability and valgus posterolateral rotary instability?
[J Am Acad Orthop Surg 2008;16:519-529]
- Varus posteromedial rotary instability injury pattern
- Coronoid fracture >15%
- Usually anteromedial facet >20%
- LCL complex avulsion
- Posterior band of MCL ruptured (anterior band intact)
- Radial head intact
2. Valgus posterolateral rotary instability injury pattern - Coronoid fracture <15% (usually tip)
- LCL complex avulsion
- Anterior band of MCL ruptured
- Radial head fracture
What are nonsurgical indications for coronoid fractures?
[JAAOS 2013;21:149-160]
- Isolated tip fractures ≤2mm
- Small fractures <15% in height with a stable elbow
What is the recommended management of anteromedial facet fractures based on O’Driscoll subtype?
[JSES (2015) 24, 74-82] [JAAOS 2013;21:149-160]
- Posterior midline incision
- AMF subtype 1 – LCL repair alone
- AMF subtype 2+3 – LCL repair and buttress plate
* T-plate, miniplate or precontoured plate - If elbow unstable after LCL and AMF fixation assess for MCL injury

What are pearls and pitfalls of the management of proximal ulnar fractures?
[JAAOS 2013;21:149-160]
Pearls
- Preoperative planning
- Stable fixation of all fragments
- Simple fractures: tension band or plate
- Complex fractures: plate and screws
- Coronoid process can be approached from medial, posterior, or lateral
- Radial head can be approached from lateral or posterior
- Fix intermediate fragments first, fix coronoid fragments distal to proximal
- Intraoperative fluoroscopy
- Test the elbow through a full ROM for stability, range, and congruence
Pitfalls
- Failure to identify and fix all fragments leads to loss of reduction or instability
- Nonanatomic reduction of the proximal ulna leads to radial head subluxation, bony impingement, and decreased motion
- Poorly placed hardware or screws and pins lead to ulnar nerve problems, decreased motion, or articular degeneration

How does proximal ulna ORIF affect elbow ROM?
[JAAOS 2013;21:149-160]
On average, patients lose 30° of ulnohumeral ROM after plate and combined plate-and-screw fixation
- ROM improves after late instrumentation removal
Which type of olecranon/proximal ulnar fixation more frequently requires hardware removal?
[JAAOS 2013;21:149-160]
Higher rate of device removal following tension band wiring (11-82%) compared with plating systems (0-20%)
- Hardware removal is most frequent complication post olecranon fixation

What are the deforming forces on a fractured clavicle?
- Distal fragment displaces inferiorly, anteriorly, medially (shortened) and rotates anteriorly
* Due to weight of arm, pectoralis major, trapezius - Proximal fragment displaces superiorly and posteriorly
* Due to SCM
What xrays should be ordered for assessing a clavicle fracture?
[J Am Acad Orthop Surg 2018;26:
e468-e476]
- AP Clavicle
- AP Clavicle with 20o of cephalic tilt
- AP Clavicle with 45o of cephalic tilt
- AP Clavicle with 45o of caudal tilt
* 45o views better for assessing AP displacement

What radiographic finding of a clavicle fracture is concerning for scapulothoracic dissociation?
[J Am Acad Orthop Surg 2018;26:
e468-e476]
Distraction of the fracture site
What is the strongest radiographic predictor of perisistent symptoms and negative sequelae post midshaft clavicle fracture?
[J Am Acad Orthop Surg 2018;26:
e468-e476]
Displacement > 1 bone width (ie, 100%)
What are the indications for clavicle ORIF?
[Rockwood and Green 8th ed. 2015]
- Fracture-specific
- Open fracture
- Impending open fracture (skin tenting)
- Shortening >2cm
- 100% displacement
- Symptomatic nonunion
- Comminution
- Segmental fractures
- Posteriorly displaced medial 1/3 fractures
- Clinical deformity/scapular malposition and winging
- Associated injuries
- Vascular injury (subclavian vein/artery) requiring repair
- Brachial plexus injury with progressive neurologic deficit
- Floating shoulder (clavicle and scapular neck fracture)
- Ipsilateral upper extremity fracture
- Multiple ipsilateral rib fractures
- Bilateral clavicle fractures
- Scapulothoracic dissociation
3. Patient factors - Polytrauma requiring early upper extremity WB
- Motivation to return to early function
- Eg. Elite athlete, self employed, etc
What are the advantages of operative treatment compared to nonop for displaced midshaft clavicle fractures?
[JBJS 2012;94:675-84][JBJS 2007;89A-1:1][JBJS 2017;99:1051-7]
- Less symptomatic nonunion
- Less symptomatic malunion
- More rapid return to function
- Improved long term function is marginal
* May not exceed minimal clinically relevant difference - Less overall complications
* Operative complications- Hardware irritation
- Wound complications
* Nonoperative complications - Nonunion
- Malunion
- Improved patient satisfaction (including cosmesis)
- Operative – scar and hardware prominence
- Nonoperative – droopy shoulder (shoulder ptosis)
- Frequency of secondary operations equal to nonoperative management (17%)
- Operative – reoperate for hardware removal
- Technically simple
- Less complications
- Short rehab
- Nonoperative – reoperate for nonunion/malunion
What is the effect of clavicle shortening post mid-shaft clavivle fracture?
[J Am Acad Orthop Surg 2018;26:
e468-e476]
Residual shortening associated with more pain and worse outcome scores
- Leads to an altered position of the scapula at rest, causing scapular dyskinesia
- Shortening as little as 10% could alter the position of the glenohumeral joint
- Shortening >14 mm in women and >18 mm in men results in worse functional outcomes scores and
decreased strength
When performing ORIF of a midshaft clavicle fracture, what is best in terms of:
Plate Size
Plate Design
Plate Position
Number of plates?
[J Am Acad Orthop Surg 2018;26:
e468-e476]
Plate Size
- 2.7 mm DCP > 3.5 mm > 2.7 mm
- Low rates of failure and nonunion
- Good outcomes
Plate Design
- Precontoured > Recon
- Similar biomechanical strength
- Decreased implant irritation, implant removal
- Improved cosmesis
- **Females and low BMI patients have increased implant irritation/removal rates, even with precontoured plates
- If superior plating is used, precontoured plating systems should be strongly considered
Plate Position
- Fracture pattern dictates implant position
- Comparable implant irritation, time to union, outcome scores
- Implant irritation decreased by robust repair of platysma covering the plate
- Advantages:
- Superior plating – tension-side of the fracture
- Anterior-Inferior plating – rotationally stronger construct, plus longer screws
Number of plates
- Dual plating techniques:
- 2.7 or 3.5mm Recon Plate placed anteroinferior + 2.0 or 2.4mm mini-frag plate placed superior
- Dual > Single
- Dual vs Superior – better at resisting superior-based loads
- Dual vs Anterior-Inferior – better at resisting anterior-based loads
- No nonunions (9% nonunion with single plating)
- Low rates of implant irritation/removal (3.7%)
What are the principles of IM nail fixation of clavicle fractures?
[J Am Acad Orthop Surg 2018;26:
e468-e476]
Typically, a nail between 2.0 and 3.5mm is used
- Goal is for IMN that is 30-40% of the midshaft medullary diameter
Timing of removal of nail is variable
- Recommended removing at 6 months
What is the rate of revision surgery post clavicle ORIF?
[J Am Acad Orthop Surg 2018;26:e468-e476]
Overall 24.6% revision surgery rate
- Most common for hardware irritation (12.7%)
- Overall implant irritation rate 3.7-40%
- Less likely with dual plating
- Females 4x more likely to have symptomatic hardware requring removal
- Avg 12 months post index surgery
- Overall implant irritation rate 3.7-40%
- Low rates of nonunion (2.6%), malunion (1.1%), and infection (2.6%)
What are the advantages and disadvantages of IM clavicle fixation?
[JAAOS 2016;24:455-464] [J Am Acad Orthop Surg 2018;26:
e468-e476]
Advantages
- Smaller incision
- Less soft tissue disruption
- Less risk to supraclavicular nerves
- Avoids subclavian vessels and brachial plexus
- Less refracture following hardware removal (compared to plates)
- Comparable time to union and outcomes compared to plate
Disadvantages
- Small clavicular canals limit use (females/small stature)
- 10% converted intraop from IMN to plate due to inability to pass the nail into the lateral aspect of the fracture
- Increased hardware irritation
- Most (all) require hardware removal
- Relative contraindication in comminuted and segmental fracture
What percent of nonsurgically managed clavicle fractures go on to symptomatic nonunion?
[J Am Acad Orthop Surg 2018;26:
e468-e476]
14-24%
What are the risk factors for clavicle nonunion?
[JSES (2013) 22, 862-868] [J Am Acad Orthop Surg 2018;26:
e468-e476]
- Clavicle shortening >15-20mm
- Female sex
- Fracture comminution
- Fracture displacement (no bony contact between fragments)
- Older age
- Severe initial trauma
- Unstable lateral fractures (Neer type II)
- Smoking
What is the NNT to avoid nonunion of displaced midshaft clavicle fractures?
[J Am Acad Orthop Surg 2018;26:
e468-e476]
- 5
* 1.7 for patients with >40% risk of nonunion
What is the management of clavicle nonunion?
[JSES (2013) 22, 862-868]
ORIF with precontoured clavicle plate
- ICBG if atrophic nonunion or bone loss
- +/- ICBG if hypertrophic nonunion
- Ensure sclerotic ends are prepared back to bleeding bone and drill the medullary canal
What is the anatomy of the coracoclavicular ligament and its function?
[JAAOS 2011;19:392-401]
- Trapezoid ligament
- lateral to the conoid ligament
- 2cm from the AC joint
- Conoid ligament
- Medial to the trapezoid ligament
- 4cm from the AC joint
- Function to prevent superior displacement of the distal clavicle in relation to the acromion
* Whereas the AC ligaments prevent horizontal displacement
What is the normal CC interspace?
[JAAOS 2011;19:392-401]
Distance between the coracoid process and the undersurface of the clavicle = 11-13mm
What is the classification of distal clavicle fractures?
[JAAOS 2011;19:392-401]
Neer classification
- Type I
- Fracture lateral to the CC ligaments
- Spares the AC joint
- Stable pattern
- Proximal fragment stabilized by the CC ligaments, distal fragment by the deltotrapezial fascia
- Often minimally displaced
- Fracture lateral to the CC ligaments
- Type II
- Proximal fragment is detached from the CC ligament
- Type IIa
- Fracture is medial to the conoid ligament
- Distal fragment remains connected to the CC ligaments (both presumed to be intact)
- Unstable (56% nonunion with nonop)
- Fracture is medial to the conoid ligament
- Type IIb
- Fracture is between the trapezoid and conoid ligament (conoid ligament is disrupted)
- Unstable (30-45% nonunion with nonop)
- Type III
- Fracture is lateral to the CC ligaments and extends into the AC joint
- Stable pattern (risk of AC arthritis)
- Type IV
- Pediatric pattern
- Epiphysis and physis remain adjacent to AC joint with fracture through the metaphysis with displacement
- Stable pattern
- Type V
- Small inferior cortical fragment remains attached to the CC ligaments
- Unstable pattern

What are the indications for nonsurgical management of distal clavicle fractures?
[JAAOS 2011;19:392-401]
- Type I
- Type II nondisplaced
- Type III
- Type IV nondisplaced

What are the indications for surgical management of distal clavicle fractures?
[JAAOS 2011;19:392-401]
- Due to high risk of nonunion due to displacement, surgery should be offered for the following types:
- Type II, displaced
- Type IV, displaced
- Type V
***NOTE: nonunion is often asymptomatic and can be managed surgically if becomes symptomatic
- Open or impending open
- Vascular injury requiring surgery

What are the described surgical options for distal clavicle fractures?
[JAAOS 2011;19:392-401]
- Described techniques:
- Transacromial wire fixation
- Modified Weaver-Dunn
- Tension band
- CC screw
- AC hookplate
- Locking plate
- Arthroscopic treatment
- ***NOTE: second procedure required for CC screw and AC hook plate for hardware removal
- JAAOS author recommendation:
* If distal fragment large:- Distal clavicle locking plate + CC stabilization with suture placed around the corocoid
* If distal fragment is small - CC stabilization with nonabsorbable suture
- 2 sutures passed around the coracoid and through drill hole in the clavicle
- Distal clavicle locking plate + CC stabilization with suture placed around the corocoid
- Simplified*
- Large distal fragment
- Distal clavicle precontoured plate
- +/- suture augmentation
- Distal clavicle precontoured plate
- Small distal fragment
- Hook plate
- CC suture stabilization
- Suture/tape alone
- Suture anchor
- Suture button
What are the complications and disadvantages of hook plate for distal clavicle ORIF?
- Hardware removal (~3 months)
- Limitation of shoulder elevation >90
- Subacromial impingement
- Rotator cuff damage/tear
- Acromion osteolysis
- Acromion fracture
- Fracture medial to the implant
- Unhooking of the plate from the acromion
What are the associated injuries with a scapula fractures?
[JAAOS 2012;20:130-141]
- Associated injuries present in 90% of patients
- Thoracic injury (80%) > ipsilateral extremity injury (50%) > head injury (48%) > spinal fractures (25%)
What are the indications for surgery for scapula fractures? [JAAOS 2012;20:130-141]
- Medial displacement of the lateral border >25mm
- Shortening >25mm
- Angular deformity >45°
- Glenopolar angle <22°
- Angle created at the intersection of a line drawn from the inferior glenoid fossa to the superior apex of the glenoid fossa and a line drawn from the superior apex of the glenoid fossa to the inferior angle of the scapula
- Normal ~30-46°
- Concomitant intra-articular step-off >3mm
- Displaced double disruption of the superior shoulder suspensory complex (SSSC)
* ‘Double disruption’ is the interruption of 2 structures in this ring resulting in an interruption in the suspension between the axial and appendicular skeleton

What are the surgical indications for scapular process fractures (corocoid and acromion)?
[JAAOS 2012;20:130-141]
- Painful nonunion
- Concomitant ipsilateral scapula fracture requiring surgery
- Displacement ≥1cm
- Two or more disruptions in the SSSC
What forms the SSSC?
[JBJS REVIEWS 2018;6(10):e5]
- Glenoid
- coracoid
- CC ligaments
- CA ligament
- Lateral end of the clavicle
- AC joint
- Acromion

What is the recommended surgical technique for scapular fractures?
[JAAOS 2012;20:130-141]
- Approaches
- Options from Posterior with patient in the lateral decubitus position
- Judet incision
- Muscular intervals = teres minor and infraspinatus
- Elevation of the deltoid, teres minor and infraspinatus is beneficial for highly comminuted fractures and in delayed ORIF
- Straight incision
- Indicated for fractures about the lateral border or isolated fractures
- Minimally invasive approach with windows directly over the site of desired plate placement
- Judet incision
- Options from Anterior with the patient in the beach chair position
- Deltopectoral approach
- Indicated for anterior glenoid fractures
- Combined or limited incision
- Indicated for disruption of the AC joint, coracoid or clavicle
2. Implant options
- Indicated for disruption of the AC joint, coracoid or clavicle
- Deltopectoral approach
- Reconstruction plates contour around the scapular spine and superomedial angle
- Dynamic compression plates provide a rigid construct that is best for the lateral border
- Precontoured implants can be used for specific scapular anatomies
What is the classification system for intra-articular fractures of the glenoid?
Ideberg (modified by Goss)
- Classified according to the location of the exiting fracture line
- Type Ia - anterior rim
- Type Ib - posterior rim
- Type II - through glenoid exiting laterally
- Type III - through glenoid exiting superiorly
- Type IV - through glenoid exiting medially
- Type Va - lateral AND medial (II + IV)
- Type Vb - superior AND medial (III + IV)
- Type Vc - lateral AND superior AND medial (II + III + IV)
- Type VI - comminuted

What is the blood supply to the humeral head?
[Rockwood and Green 8th ed. 2015]
- Posterior humeral circumflex artery gives off metaphyseal branches to the posteromedial proximal humerus
* Recent cadaver study demonstrated the posterior humeral circumflex artery provides 64% of blood supply to the humeral head [JBJS 2010;92:943-8] - Anterior humeral circumflex artery gives off the ascending branch (courses lateral to bicipital groove) to form the arcuate artery just below the articular surface
What is the proximal humerus orientation?
- Humeral retroversion = avg 30o retroversion
* With respect to the humeral epicondyles - Humeral head inclination with respect to the shaft = avg 130o

What is the Neer classification of proximal humerus fractures?
- Based on number of parts (1-4)
- Articular surface
- Greater tuberosity
- Lesser tuberosity
- Shaft
- A separate part is determined if there is >45 degrees angulation or >1cm displacement

What are the risk factors for humeral head AVN following proximal humerus fracture?
[J Shoulder Elbow Surg. 2004;13(4):427-33]
- Strong predictors
- Posteromedial metaphyseal head extension <8mm
- Disruption of the medial hinge
- >2mm of shaft displacement in any direction
- Only relevant if posteromedial metaphyseal head extension <8mm
- Anatomic neck fractures
2. Moderate to strong predictors - 4-part fractures
- Angular displacement of the head >45°
- Displacement of tuberosities >10mm
- Glenohumeral dislocation
- Head split
- 3-part fractures
- Medial (vs. lateral) shaft displacement

In general, what are the indications for nonoperative management of proximal humerus fractures?
[Rockwood and Green 8th ed. 2015]
- Stable nondisplaced or minimally displaced fractures
- Patients not fit for surgery
- Elderly patients with low functional demands
What are two ways to determine stability of proximal humerus fractures?
[Rockwood and Green 8th ed. 2015]
- Radiographically
- Impaction and interdigitation of fragments
- Eg. valgus-impacted fracture with impaction of anatomical neck into the metaphysis
- Clinically
* Palpation of proximal fragment with rotation of the arm will result in fragments moving as a unit and feeling of crepitation (due to bony contact) if stable
In general, what are surgical indications for proximal humerus fractures?
[Journal of Orthopaedic Surgery and Research (2017) 12:137]
- Three- or four-part fracture dislocations
- Head split fractures
- Pathological fractures
- Open fractures
- Associated neurovascular injury
- Displaced two-part surgical neck fractures
- >5mm displacement of greater tuberosity fracture
- Displaced 3-part fractures
- Displaced 4-part fracture in young patient
What are the operative options for proximal humerus fractures?
[JAAOS 2017;25:42-52]
- CRPP
- IM nail
- Plate
- Hemiarthroplasty
- rTSA
What is the most common reason for varus collapse and what are 4 ways to prevent varus displacement?
[Journal of Orthopaedic Surgery and Research (2017) 12:137]
- Loss of medial calcar support
4 ways to prevent varus displacement include:
- Anatomic reduction of the medial cortices if no comminution
- Inferomedial calcar screw
- Oblique locking screw in the inferomedial quadrant of the head
- Head-on-shaft impaction
- Can be achieved with a valgus impaction osteotomy
- Fibular strut allograft
What are the indications for surgical fixation of a greater tuberosity fracture?
[J Am Acad Orthop Surg 2016;24:46-56]
5mm of superior displacement in healthy population
- Consider 3mm displacement if patient requires prolonged overhead activity
What is the direction of displacement of the GT fragment and why?
[J Am Acad Orthop Surg 2016;24:46-56]
Superior and posterior due to pull of supraspinatus, infraspinatus and teres minor
What is the direction of displacement of the LT fragment and why?
[J Am Acad Orthop Surg 2012;20:17-27]
Anterior and medial due to pull of subscapularis
What is the direction of displacement of the shaft fragment and why?
[J Am Acad Orthop Surg 2012;20:17-27]
Adducted and anteriorly displaced due to pull of pectoralis major
What are 3 GT fracture patterns (proximal humerus) and what surgical options can be employed?
[J Am Acad Orthop Surg 2016;24:46-56]
- Avulsion
- Small fragment with a horizontal fracture line relative to the long axis of the humerus
- Arthroscopic or mini-open deltoid split utilizing double-row suture anchor repair or transosseous fixation techniques
- Split
- Large fragment with a vertical fracture line relative to the long axis of the humerus
- Arthroscopic or mini-open deltoid split utilizing double-row suture-bridge, interfragmentary compression screws, or a small locking plate augmented with sutures through the RC tendon
- Depression
- Inferiorly displaced and impacted GT
- Nonop
What are the indications for plate osteosynthesis for proximal humerus fractures?
[JAAOS 2017;25:42-52]
- Displaced 2-part fractures
- 3 part fractures without significant comminution
- 4 part fractures in active patients <65 with acceptable bone stock and minimal comminution
What are the principles of proximal humerus ORIF with locking plate?
[Rockwood and Green 8th ed. 2015]
- Beach chair position with C-arm from head of bed
- Deltopectoral approach (start 1-2cm lateral to corocoid)
- Place sutures in the supraspinatus and infraspinatus to control the greater tuberosity and in the subscapularis to control the lesser tuberosity
- Reduce the humeral head by correcting varus/valgus displacement
- Reduce the tuberosities
- Provisional K-wire fixation
- Confirm reduction on AP and lateral views
- Place locking plate posterior to the bicipital groove and sufficiently inferior to avoid impingement
* 5-8mm distal to top of GT - Thread RC sutures through proximal plate prior to plate fixation
- Place two locking screws proximally and one distal
* This allows final correction in the sagittal plane - Place final locking screws in head (usually 5) and final distal screws (usually 3)
- Tie RC sutures to plate
- Under live fluoro confirm screw length, no intra-articular perforation and no impingement
What are the complications associated with plate osteosynthesis of proximal humerus fractures?
[JAAOS 2015;23:190-201]
- Screw penetration (most common)
- Screw cutout (loss of fixation)
- Varus collapse
- Plate impingement
- Osteonecrosis
What are the indications for IM nail for proximal humerus fractures?
[JAAOS 2017;25:42-52]
- 2 part surgical neck fractures
- Concomitant humeral shaft fracture
- Impending pathological fracture
- Select 3 and 4 part fractures
What are the advantages and disadvantages of a more medial start point compared to a more lateral start point for humeral IMN?
[Rockwood and Green 8th ed. 2015][JSES (2016) 25, e130–e138]
More medial (typical of straight nails)
- Advantages
- Avoids supraspinatus tendon
- Better healing of supraspinatus muscle (compared to tendon)
- Theoretically less rotator cuff tendinopathy (and less pain)
- Avoids supraspinatus tendon
- Disadvantages
- Articular cartilage damage
More lateral (typical of nails with proximal lateral bend)
- Advantages
- Avoids articular cartilage
- Disadvantages
- Supraspinatus tendon damage
What are the indications for hemiarthroplasty in proximal humerus fractures?
[JAAOS 2012;20:17-27]
- Intial varus malalignment >20° in whom anatomic reduction can not be achieved intraoperatively
- Moderate or severe osteopenia
- Age >55 with 3 or 4 part fracture dislocations or head split
- Malunion
- Nonunion
- Hardware failure
- Osteonecrosis of humeral head following osteosynthesis
What are the critical components of successful shoulder hemiarthroplasty?
[JAAOS 2012;20:17-27]
- Tuberosity position and healing
- Bone graft from humeral head applied between the prosthesis and tuberosities
- Tuberosities are sutured to each other, to the shaft through drill holes, to the lateral fin, and a medial cerclage suture around the prosthesis
- Final tensioning of the sutures should be done with arm slightly flexed and neutral to slight external rotation
- Rotator interval is closed with arm in neutral to slight external rotation
2. Humeral height - Place top of humeral head prosthesis 56mm proximal to the superior border of pectoralis major tendon
- GT and LT fragments should reduce anatomically under minimal tension at the prosthetic interface
- Humeral head version
- Recommended 20-30° retroversion
- References
- Bicipital groove
- Place the lateral fin of the prosthesis 30° posterior to the posterior margin of the bicipital groove
- Transepicondylar axis (forearm)
- Bicipital groove
What are ways to assess proper height of shoulder hemiarthroplasty?
- The pectoralis major tendon should be 5.6cm below the height of the top of the humeral head
- Appropriate soft tissue tension of deltoid and long head of biceps
- Top of humeral head relative to superior glenoid
- Top of prosthesis relative to GT
* Head should be 5-16mm proximal to the GT - Top of humeral head relative to inferior acromion
* (?fingerbreadth)
What features of the hemiarthroplasty prosthesis are important?
[JAAOS 2017;25:42-52]
Modular stem convertible to a rTSA
What is the unhappy shoulder triad?
[JAAOS 2012;20:17-27]
Prosthesis:
- Too proud
- Too retroverted
- GT too low
Leads to posterior migration of the GT and poor function
What is the main determinant of outcome with shoulder hemiarthroplasty?
[JAAOS 2015;23:190-201]
Tuberosity union
What are the indications for reverse total shoulder arthroplasty for proximal humerus fractures?
[JAAOS 2017;25:42-52] [JAAOS 2015;23:190-201]
- Age >65 (>70) with 3 and 4 part fractures
- Relative indications
- Risk factors for inferior functional results from plate osteosynthesis or hemiarthroplasty
- Irreparable fracture
- High risk of osteonecrosis
- Poor tuberosity bone quality
- Osteoporosis and/or comminution
- Preexisting chronic RTC tear
- Preexisting arthritis
- Prerequisites
- Functioning deltoid (axillary nerve)
- Adequate glenoid bone stock
What are contraindications for rTSA in proximal humerus fracture?
[JAAOS 2015;23:190-201]
Absolute
- Permanent axillary nerve dysfunction
- Global deltoid dysfunction
- Global brachial plexopathy
How do you assess the soft tissue tension in rTSA?
[JAAOS 2015;23:190-201]
- Axial shuck test
- Axial traction on adducted humerus
- Optimal is 1-2mm of gapping
- Lateral instability
- Lateral dislocation force applied with one finger on calcar
- Assess ease of dislocation/subluxation
- Adduction deficit
- Gravity adduction
- Due to overlengthened humerus or glenoid baseplate too superior
- Strap muscle tightness
* In neutral extension should contribute to joint compression
How can you adjust the soft tissue tension in rTSA?
[JAAOS 2015;23:190-201]
- Increase polyethylene size
- Implant humeral stem proud or deep
- Change glenosphere diameter
- Lateralize the glenosphere
What is the importance of tuberosity union in rTSA?
[JAAOS 2015;23:190-201]
Improved external rotation
***Note
- In both hemiarthroplasty and rTSA, healing of the GT leads to superior clinical outcomes
- However, in rTSA healing of the GT is not a prerequisite for a good outcome
What is scapular notching and what are the predictors of notching?
[JAAOS 2015;23:190-201]
- Radiographic finding likely due to contact between the scapular neck and polyethylene during adduction
- Associated with:
- Loss of baseplate fixation
- Poor patient outcomes
- Is an independent risk factor for failure
- Predictors of notching include:
- Superior position of glenosphere
- Medialization of the centre of rotation
- High BMI
What is the definition of a scapulothoracic dissociation?
[JAAOS 2017;25:339-347]
- Characterized by lateral displacement of the scapula due to traumatic disruption of the scapulothoracic articulation
- Involves a spectrum of osseous, muscular, vascular and neurologic injuries
- Intact overlying skin is a feature
In order for lateral scapular displacement to occur (in scapulothoracic disocciation), what structures must be affected?
[JAAOS 2017;25:339-347]
SC joint and/or Clavicle fracture and/or AC joint
- Most commonly associated with a distracted clavicle fracture
In what order is it thought that structures fail in scapulothoracic dissociation?
[JAAOS 2017;25:339-347]
Musculoskeletal → vascular → neurologic
What is the characteristic sign of an associated vascular injury in scapulothoracic dissociation?
[JAAOS 2017;25:339-347]
Pulselessness
What type of neurological injury occurs to the nerve roots in scapulothoracic dissociation?
[JAAOS 2017;25:339-347]
- Preganglionic – limited healing potential
- Postganglionic – greater healing potential
What radiographic features are used to diagnose a scapulothoracic dissociation on a CXR?
[JAAOS 2017;25:339-347]
- Increased soft tissue density in vicinity of scapula (hematoma)
- Distraction of a clavicle fracture, AC joint or SC joint
- Scapular lateralization
- Measure distance between thoracic spinous process to medial border of scapula at the same level for both injured and uninjured sides
- Scapular index = injured distance/uninjured distance
- >1.29 is scapulothoracic dissociation until proven otherwise
- Difference >1cm is consistent with scapulothoracic dissociation
- Scapular index = injured distance/uninjured distance
What other imaging modality can be considered in scapulothoracic disocciation?
[JAAOS 2017;25:339-347]
- Convential angiogram
- CT myelography
- Identifies pseudomeningocele and preganglionic nerve injury
- Perform >3 weeks after injury
- Allows time for blood clot to resorb and pseudomeningocele to form
- MRI
* Most effective for postganglionic nerve injury - EMG/NCV
* Initially performed at 3-4 weeks postinjury then every 6 weeks to monitor recovery
What is the classification system for scapulothoracic dissociations?
[JAAOS 2017;25:339-347]
Zelle Classification
- Type 1 - isolated MSK injury
- Type 2A - MSK and vascular injury
- Type 2B - MSK and incomplete neurological injury
- Type 3 - MSK, vascular and incomplete neurological injury
- Type 4 - MSK injury and complete brachial plexus avulsion
What is the management of scapulothoracic dissociations?
[JAAOS 2017;25:339-347]
- Vascular injury determines the urgency of surgery
- In presence of a vascular injury requiring repair:
- Generally the orthopedic injury (clavicle fracture, AC or SC injury) is repaired to protect the vascular repair
- Upper extremity fasciotomies are performed
- If no vascular injury the orthopedic injuries are dealt with when patient condition allows
- Orthopedic injuries
- Fixation is often redundant due to the severe soft tissue injuries requiring increased stabilization
- Clavicle fracture – dual orthogonal plating
- AC joint – hook plate with CC screw and anterior plating across AC joint
- SC joint – reconstructed with allograft or autograft tendon
- Neurological injuries
- Generally delayed
What are the outcomes following scapulothoracic injuries?
[JAAOS 2017;25:339-347]
- 52% = flail extremity
- 21% = early above elbow amputation
- Outcome largely determined by the neurological injury
What is the classification of humeral shaft fractures?
AO/OTA classification
- Simple fractures (type A)
- Wedge fractures (type B)
- Complex fractures (type C)

What landmarks define the humeral shaft?
[JAAOS 2012;20:423-433]
- Superior border of pectoralis major
- Supracondylar ridge
What are acceptable alignment paramaters for nonoperative management of humeral shaft fractures?
[AAOS comprehensive review 2, 2014]
30° varus/valgus angulation
20° AP angulation
15° rotation
3cm of shortening
What are indications for surgical treatment of humeral shaft fractures?
[Rockwood and Green 8th ed. 2015]
Absolute indications
- Unacceptable alignment by closed means
- Polytrauma
- Bilateral humeral shaft fractures
- Floating elbow
- Intra-articular extension
- Progressive nerve palsy or nerve palsy after closed manipulation
- Vascular injury requiring repair
- Neurologic deficit after penetrating injury
- Nonunion
- Pathologic fracture
- Skin condition precludes bracing (eg. burns)
- High velocity gun shot wounds
Relative indications
- Open fractures
- Segmental fractures
- Noncompliant patients
- Obesity or large breasts
- Periprosthetic fractures
- Transverse or oblique middle 1/3 fractures
- Long oblique fracture of the proximal 1/3
What is the nonoperative management of humeral shaft fractures?
Coaptation splint or hanging cast for 5-7 days
- Followed by functional bracing (Sarmiento) and cuff-and-collar
- Coaptation splint should be as high up in the axilla as possible and over the deltoid, molded into valgus
- Functional bracing allows elbow and wrist ROM, shoulder ROM should be avoided until fracture is stable
What patient and fracture characteristics are more prone to nonunion in humeral shaft fractures?
[J Shoulder Elbow Surg (2017) in press]
- Proximal 1/3 fractures
- Oblique pattern in the proximal 1/3
- Increasing fracture gap size
- Smoking
- Female
What are the surgical treatment options for humeral shaft fractures?
[Rockwood and Green 8th ed. 2015]
- ORIF with plate
- Most treated with 4.5mm LC-DCP with 3-4 bicortical screws above and below
- Lag screw if possible in simple fractures or as bridge plate in comminuted fractures
- IM nail (antegrade/retrograde)
- External fixation
What are the surgical approaches for humeral shaft fractures?
[Rockwood and Green 8th ed. 2015] [JAAOS 2012;20:423-433]
- Anterolateral for proximal 2/3 fractures
* Identify the musculocutaneous nerve deep to biceps and radial nerve between brachialis and brachioradialis - Posterior approach for distal 1/3 fractures
* Document location of radial nerve relative to plate if a posterior approach is utilized
What humeral shaft fracture characteristics are more commonly associated with radial nerve palsy?
[JAAOS 2012;20:423-433]
- Distal fractures > proximal fractures
- Transverse and spiral fractures > comminuted or oblique
NOTE: no difference between open or closed
What are the indications for radial nerve exploration in the setting of humeral shaft fracture?
[JAAOS 2012;20:423-433]
- Open fracture
- High-velocity gunshot or penetrating injury
- Vascular injury
- Nerve deficit after closed reduction (controversial)
- Distal third (Holstein-Lewis) fracture (controversial)
What are the indications for humeral IM nail?
[JBJS REVIEWS 2015;3(9):e5]
- Comminution
- Segmental fractures
- Pathological fractures
What are the disadvantages of IM nail for humeral shaft fractures?
[Medicine (Baltimore). 2015 Mar;94(11):e599]
- Shoulder pain and impingement
- Reoperation for hardware removal
Note – no difference in fracture union, radial nerve injury, and infection
What is the classification for distal humerus fractures?
[AAOS comprehensive review 2, 2014] [Miller’s, 6th ed.]
- Intra-articular fractures
- Single-column fractures
- Medial (high/low)
- Lateral (high/low)
- Divergent
- Two-column fractures
- Jupiter classification
- High T
- Proximal or at level of olecranon fossa
- Low T
- Through olecranon fossa
- Y pattern
- Oblique portion through both columns
- H pattern
- Trochlea is detached from medial and lateral columns
- Medial lambda
- Proximal fractures exits medial
- Lateral lambda
- Proximal fracture exits lateral
- High T
- Jupiter classification
- Capitellar fractures
- Trochlear fractures
2. Extra-articular/intracapsular - High transcolumnar fracture
- Extension
- Flexion
- Abduction
- Adduction
- Low transcolumnar fracture
- Extension
- Flexion
- Extra-capsular fractures
- Medial epicondyle
- Lateral epicondyle

What are the O’Driscoll Principles of distal humerus fracture fixation to optimize stability?
[JSES. 2005;14(1 Suppl S):186S-194S]
- To prevent failure at the supracondylar level through loss of fixation in the distal fragments and thereby maximize the potential for union and full elbow mobility after a severely fractured distal humerus, 2 principles must be satisfied:
* Fixation in the distal fragment must be maximized
* All fixation in distal fragments should contribute to stability between the distal fragments and the shaft. - There are 8 technical objectives by which these principles are met:
- Every screw in the distal fragments should pass through a plate
- No screws are placed in the distal fragments before application of plates (use k-wires)
- Engage a fragment on the opposite side that is also fixed to a plate
- As many screws as possible should be placed in the distal fragments
- Each screw should be as long as possible
- Each screw should engage as many articular fragments as possible
- The screws in the distal fragments should lock together by interdigitation, creating a fixed-angle structure
- Plates should be applied such that compression is achieved at the supracondylar level for both columns
- The plates must be strong enough and stiff enough to resist breaking or bending before union occurs at the supracondylar level
- Practically:
- Use of “parallel” plates that permit at least 4-6 long screws to be placed in the distal fragments, from one side across the other
- Ccrews placed at the epiphyseal level interlock, increasing the stability of the construct
- The plates must be contoured or precontoured to
the normal geometry of the distal humerus to allow
screw placement at the appropriate places and also not to be too prominent under the skin- Precontoured plates easier and more consistent

In a complex distal humerus fracture with missing bone, what 2 principles should be considered when reconstructing the articular surface?
[JSES. 2005;14(1 Suppl S):186S-194S]
- The anterior aspect of the distal humerus is the critical part of the articulation that needs to be fixed in order to have a functional joint
- Stability of the articulation requires the medial trochlea and either the lateral half of the trochlea or the capitellum
* Medial trochlea is essential for stable, well-aligned joint

In a complex distal humerus fracture what are 2 techniques for fixation of the metaphyseal region?
[JSES. 2005;14(1 Suppl S):186S-194S]
- Anatomic reconstuction (preferred)
- Supracondylar shortening
- Humerus can be shortened at the metaphyseal fracture site, provided that the overall alignment and geometry of thedistal humerus are restored
- Shortening by 1 cm or less creates no apparent loss of function,
- Up to 2cm of shortening can be tolerated without serious disturbance of elbow biomechanics
What is the name of a distal 1/3 humeral shaft spiral fracture commonly associated with radial nerve palsy (22%)?
Holstein-Lewis fracture
What are options for the posterior approach to the distal 1/3 of the humerus?
***Note: all involve universal posterior midline incision and raising full thickness medial and lateral fasciocutaneous flaps with identification and protection of the ulnar nerve
- Paratricipital
- Tricep split
* Useful for open fractures as there is often a defect in the triceps - Olecranon osteotomy [J Am Acad Orthop Surg 2010;18:20-30]
- Pros:
- Best articular exposure
- Allows early range of motion
- Cons:
- Nonunion
- Stiffness
- Symptomatic hardware
- Triceps peel
- Triceps turn down
Describe the anatomy of the radial nerve, as encountered during posterior approach to the humerus
[JBJS 1996 Nov;78(11):1690-5.]
- Location from distal humerus
- 20.7 ± 1.2cm proximal to the medial epicondyle
- 74% of the length of the humerus
- 14.2 ± 0.6cm proximal to the lateral epicondyle
- 51% of the length of the humerus
- Pierces lateral intermuscular septum 10.2 ± 0.4cm proximal to the lateral epicondyle
- 36% of the length of the humerus
- Branches
- Multiple to lateral head of triceps
- None to medial head of triceps until nerve crosses lateral aspect of humerus
- Trifurcates at lateral aspect of humerus:
- Branch to medial head of triceps
- Lower lateral brachial cutaneous nerve
- Find and trace proximally to find radial nerve proper
- Continuation of radial nerve to forearm
What approach provides the greatest exposure to the posterior humeral shaft?
[JBJS 1996 Nov;78(11):1690-5.]
- Gerwin approach
- Medial and lateral triceps heads along with the radial nerve are mobilized lateral to medial off the humeral shaft
- Lateral intermuscular septum is divided distally to allow mobilization of the radial nerve
- The percentage of posterior humerus exposed for the 3 compared approaches:
- 94% = Gerwin approach
- 76% = Triceps split with superior mobilization of the radial nerve and lateral head of triceps
- 55% = Triceps split
- The limiting structure of each approach is:
- Gerwin = Axillary nerve
- Triceps split with radial nerve mobilization = Radial nerve branch to medial head of triceps
- Triceps split = Radial nerve

What are the principles of ORIF for two-column distal humerus fractures?
[J Am Acad Orthop Surg 2010;18:20-30]
The goal of ORIF is to anatomically reconstruct the elbow joint with a rigid construct that allows for early ROM
- First, reconstruct the articular segment
* Lag fragments together provisionally with threaded k-wires - Second, attach the articular segment to a column converting a complete articular fracture to a partial articular fracture
- Third, dual plating with precontoured periarticular distal humerus locking plates oriented perpendicular (“90-90”) or parallel while observing O’Driscoll’s principles
* Parallel plating is the strongest construct - Fourth, once fixation complete assess elbow through ROM to assess for hardware impingement
What is the recommended post-operative care following ORIF of distal humerus fractures?
J Am Acad Orthop Surg 2010;18:20-30]
- Splint at 30-40°flexion and neutral rotation
- Immediate hand, wrist and shoulder ROM
- Elbow ROM exercise started 7-10 days postop if fixation stable
* If questionable stability max delay is 3 weeks - Resistance exercise started following radiographic evidence of healing (8-12 weeks)
What are complications of distal humerus fracture ORIF?
[J Am Acad Orthop Surg 2010;18:20-30] [JSES. 2005;14(1 Suppl S):186S-194S]
- Elbow stiffness
* From prolonged immobilization used to compensate for inadequate fixation - Loss of terminal extension
- HO
- Loss of fixation
* Nonunion at supracondylar level - Nerve injury
- Infection
What is the best management of the ulnar nerve during distal humerus ORIF?
[Hand Clin. 2018 Feb;34(1):97-103]
- Based on a meta-analysis the incidence of ulnar nerve neuropathy is:
- 15.3% = in situ release
- 23.5% = transposition
- COTS trial (2017)
* No difference with regards to ulnar nerve symptoms, functional outcomes, or complications for patients treated with either simple decompression or anterior transposition of the ulnar nerve
When should a total elbow arthroplasty be considered in distal humerus fractures?
[J Am Acad Orthop Surg 2010;18:20-30]
Comminuted intra-articular fractures in the elderly and in patients with RA
What are the advantages of TEA in comminuted and osteoporotic distal humerus fractures?
[COTS 2009]
Compared to ORIF, TEA resulted in:
- Significantly better Mayo Elbow Performance Score (MEPS) at two years
- Superior DASH scores during early follow-up assessments
These positive results were also accompanied by a trend towards fewer revision surgeries.
What is the Bryan-Morrey classification of capitellar fractures?
[Hand Clin 31 (2015) 615–630]
Type 1 - (Hahn-Steinthal)
- Involves a fracture isolated to the capitellum with attached subchondral bone
Type 2 - (Kocher-Lorenz)
- Involves primarily the articular cartilage overlying the capitellum (little subchondral bone)
Type 3 - (Broberg-Morrey)
- Comminuted capitellum fractures
Type 4 - (McKee)
- Involves a capitellum fracture that extends medially into the trochlea

What are common injuries associated with capitellum fractures?
[Hand Clin 31 (2015) 615–630]
- Radial head fracture
- LCL disruption
- Elbow dislocation
What are the recommended surgical treatment options for capitellar fractures?
[Hand Clin 31 (2015) 615–630]
Type I (large subchondral fragment)
- Two cannulated partially threaded screws inserted P-A perpendicular to fracture plane
Type II (lacks subchondral bone)
- Cannulated headless compression screw inserted A-P
Type III (comminuted)
- Small fragment fixation may be achieved with the use of countersunk finethreaded k-wires
- Bone defects filled with bone graft (ICBG or synthetic) and/or augmented with locking posterolateral plate fixation
What are potential complications following ORIF of capitellum fractures?
[Hand Clin 31 (2015) 615–630]
- Elbow stiffness
- Posttraumatic arthritis
- Nonunion
- Heterotopic bone formation
- Avascular necrosis
- Painful hardware
- Intra-articular hardware
- Failure of fixation
What are complications of forearm fractures?
- Infection
- Malunion
- Nonunion
- Radioulnar synostosis
- Re-fracture
- Compartment syndrome
What is the axis of forearm rotation (pronation/supination)?
[JAAOS 2017;25:e150-e156]
Line connecting the center of the radial head and ulnar head
What is a method to assess the radial bow?
[JAAOS 2014;22:437-446] [J Bone Joint Surg. 1992;74-A:1068–78]
- On an AP radiograph a line is drawn from the radial tuberosity to the most ulnar edge of the distal radius, from this line the longest possible perpendicular line is drawn to the radius
- Normal = 15.3+/-0.3mm
- Patients with 80% rotation of the normal forearm have a radial bow of 15+/-1.5mm
* I.E. within 1.5mm of the well side

Where is the radial bow located along the radial shaft?
[J Bone Joint Surg. 1992;74-A:1068–78]
60% of the distance from the radial tuberosity to the ulnar edge of the distal radius

What order should the radius and ulna be fixed in a both bone forearm fracture?
[JAAOS 2014;22:437-446]
- Bone with less comminution to restore length
- If no comminution start with the radius
* Creates a rigid forearm to fix the ulna with the elbow flexed
What approach should be used to fix the radius and ulna in a forearm fracture?
[JAAOS 2014;22:437-446]
- Proximal radius:
* Thompson approach (ECRB and EDC) – debatable - Distal radius:
- Volar Henry approach
- FCR and BR distally and pronator teres and BR proximally
- For plating, requires elevation of:
- Pronator quadratus
- FPL
- FDS
- Pronator teres
- Pronation allows access to insertion
- Supinator
- Supination allows access to insertion
3. Ulna:
- Supination allows access to insertion
- Subcutaneous border between FCU and ECU
What construct should be used for fixation of both bone forearm fractures?
[JAAOS 2014;22:437-446]
- 3.5mm compression plate
- Goal is to restore length, alignment, rotation and radial bow
- Distal ulna fractures can be fixed with two 1/3 semitubular plates perpendicular (90-90) to avoid implant prominence
What is the postoperative management of both bone ORIF?
[JAAOS 2014;22:437-446]
- Immediate ROM of fingers
- Forearm rotation after 5-7 days
- Return to most activities by 3 months
What are the principles of treatment for late instability following ORIF of a trans-olecranon fracture dislocation?
[JBJS REVIEWS 2014;2(1):e3]
- Restoration of an anterior coronoid process buttress for the trochlear notch
- Recognition of the contribution of competent collateral ligamentous complexes in late instability
- Restoration of radiocapitellar contact
What is a transolecranon fracture dislocation?
[JBJS REVIEWS 2014;2(1):e3]
A proximal ulnar fracture at the greater sigmoid notch and anterior dislocation of the elbow, without disruption of the PRUJ
What are risk factors for developing radioulnar synostosis?
- Trauma-related
- Radius and ulna fracture at the same level
- Monteggia fracture
- High energy with significant comminution
- Significant soft tissue injury/open fracture
- Head trauma
2. Treatment-related - Use of bone graft
- Single incision approach
- Screws that penetrate the interosseous membrane
- Delayed surgery (>2 weeks)
- Prolonged immobilization
What is a monteggia fracture?
[JAAOS 2013;21:149-160]
Proximal ulna fracture with radial head dislocation
- Disruption of the PRUJ
What is the classification system for Monteggia fractures?
[JAAOS 2013;21:149-160] [JBJS REVIEWS 2014;2(1):e3]
- Bado classification
- Type I
- Anterior dislocation of the radial head with an anterior angulation of the proximal ulna fracture
- Mechanism = pronation injury
- 60% - most common in kids, young adults
- High energy injury in adults with higher rate of NV complications
- Type II
- Posterior dislocation of the radial head with a posterior angulation of the proximal ulna fracture
- 15% - makes up 70-80% of adult Monteggias
- Low energy injury
- Assoc with radial head/coronoid fractures and ligament disruption
- Coronoif process or radial head fracture is poor prognostic factor
- Type III
- Lateral or anterolateral radial head dislocation associated with a proximal ulna fracture
- 20%
- Type IV
- Anterior dislocation of the radial head with fractures of the proximal ulna and radius
- 5%
- Jupiter modification of type II
- Type IIA
- Fractures through the greater sigmoid notch and involve the coronoid
- Type IIB
- Fractures distal to the coronoid and at the proximal metaphysis
- Type IIC
- Diaphyseal fractures
- Collateral ligamentrs typically spared
- Diaphyseal fractures
- Type IID
- Comminuted proximal ulna fractures
- Involve coronoid and olecranon
- Comminuted proximal ulna fractures

What are the keys to surgical management of Monteggia fractures?
[Orthop Clin N Am 44 (2013) 59–66]
- Anatomic reduction of the ulna
- Evaluate for associated injuries
- Commonly LUCL, coronoid and radial head
- Olecranon fracture creates an ‘osteotomy’ to work through to fix the coronoid and occasionally the radial head
- Kocher interval can be used to address radial head if not accessible
- LUCL is repaired last
What must be considered if the radial head remains subluxed after ulna fixation when treating a Monteggia fracutre?
- Nonanatomic ulna fixation
* Address by correcting alignment and fixation of ulna - Interposed soft tissue in radiocapittelar joint
* Address by doing a lateral approach and removing interposition
What structures can block radial head reduction (in Monteggia)?
[JSES Open Access 1 (2017) 85–89]
- Annular ligament
- Capsule
- PIN
- Distal biceps tendon (lateral to radial head)
- Brachialis (button hole through)
What is the most common nerve injury associated with Monteggia fractures?
[Orthobullets]
PIN palsy
What is a Galeazzi fracture?
[J Am Acad Orthop Surg 2011;19:623-633]
Distal radius shaft fracture with disruption of the DRUJ
- Fracture is usually at the junction of distal and middle 1/3

At what distance from the lunate facet of the distal radius are radius fractures most likely to cause disruption of the DRUJ?
[J Am Acad Orthop Surg 2011;19:623-633]
Fractures of the radius within 7.5cm of the lunate facet appear to be at greatest risk of DRUJ disruption
What is the primary stabilizer of the DRUJ?
[J Am Acad Orthop Surg 2011;19:623-633]
The TFCC and its palmar and dorsal radioulnar ligaments

What are the deforming forces on the distal radius in Galeazzi fractures?
[J Am Acad Orthop Surg 2011;19:623-633]
- Pronator quadratus = rotational (pronation)
- Brachioradialis = shortening
- APL and EPB = shortening

What is the Walsh Classification for Galeazzi fractures?
[J Am Acad Orthop Surg 2011;19:623-633]
Type 1
- Apex volar
- Distal radius displaces dorsal and distal ulna displaces volar
- Mechanism – typically axial load and supination
Type 2
- Apex dorsal
- Distal radius displaces volar and distal ulna displaces dorsal
- Mechanism – typically axial load and pronation
- 73% of pediatric Galeazzi fractures

What is a Galeazzi-equivalent lesion?
[J Am Acad Orthop Surg 2011;19:623-633]
A variant of the classic Galeazzi fracture seen in skeletally immature children and adolescents
- Characterized by fracture of the radius with fracture through the distal ulna physis but without disruption of the DRUJ
- The distal epiphysis separates, but the ligamentous
restraints of the DRUJ do not rupture- Epiphyseal plate is biomechanically weaker than the ligamentous complex that stabilizes the DRUJ
- Usually managed non-op with closed reduction and long arm cast
- May need ORIF if soft-tissue interposition blocks reduction
What are the radiographic features that would suggest a DRUJ injury?
[J Am Acad Orthop Surg 2011;19:623-633] [The Journal of Hand Surgery (European) 2014, 39E(7) 727–738]
- Fracture of the ulnar styloid base
* Controversial in recent literature - Widening of the DRUJ on the AP view
- Most predictive of instability on XR
- A 1% increase in the radial translation ratio (widening of the DRUJ gap by approximately 0.25 mm in a typical individual) associated with a 50% increased risk of instability
- Dislocation/subluxation of the radius relative to ulna on true lateral view
- Shortening of the radius >5mm relative to the distal ulna
* Indicates likely injury to TFCC or IOM - Asymmetry compared to the contralateral DRUJ
What is the treatment algorithm for Galeazzi fractures?
[J Am Acad Orthop Surg 2011;19:623-633]
- Adults require ORIF with LC-DCP plate achieving anatomic reduction of distal radius followed by intra-operative assessment of the DRUJ
* Confirm reduction on AP and lateral views followed by assessment of stability in supination and pronation - DRUJ is then characterized as reduced and stable, reduced and unstable, irreducible
- Reduced and stable = protective splint and early motion
- Reduced and unstable = assess for large ulnar styloid fracture OR TFCC tear
- None present = K-wire fixation ulna to radius
- Ulnar styloid fracture = ORIF with lag screw, tension band or K-wire
- TFCC tear = avulses from base of ulnar styloid requiring repair with drill holes or suture anchors
- Then fix DRUJ with two 1.6mm K-wires ulna to radius with forearm in supination
- Irreducible = surgical exploration to remove block (ECU or fracture fragments)
- Then reassess and treat as stable or unstable DRUJ

What injuries are associated with distal radius fractures?
[Rockwood and Green 8th ed. 2015]
- Carpal interosseous ligaments
* Scapholunate and lunotriquetral - TFCC
- Chondral lesions
What are risk factors for re-displacement following closed reduction of distal radius fractures?
[Rockwood and Green 8th ed. 2015]
- Increasing age
- Greater degree of initial displacement
- Metaphyseal comminution
- Prior failure of closed reduction
What are the radiographic features that should be evaluated on a PA wrist and lateral wrist radiograph in context of distal radius fracture?
[Hand Clin 21 (2005) 279–288]
- PA wrist
- Carpal facet horizon
- With volar tilt of articular surface, transverse radiodense line represents the volar rim of the lunate facet because the XR beam is parallel to the subchondral bone of volar rim
- With dorsal tilt of articular surface (i.e. fracture), transverse radiodense line represents the dorsal rim of the lunate facet because the XR beam is parallel to subchondral bone of the dorsal rim
- Radiocarpal interval (joint space)
- Normal ~2mm (<3mm)
- Measure radial height and inclination from the midpoint between volar and dorsal ulnar corner (central reference point)
2. Lateral wrist - True lateral view = pisiform overlaps the distal pole of the scaphoid and is volar to the capitate head
- Pisiform dorsal = pronation
- Pisiform volar = supination
- Congruent distal radius and lunate articular surface (matched radius of curvature)
- Colinear lunate and distal radius
- Tear drop angle
- Best assessed on 10° lateral view
- Lift hand 10o or point beam 10o proximal
- The teardrop represents the volar rim of the lunate facet
- Angle formed between line along central axis of the teardrop and a line along the central axis of the radial shaft
- Normal = 70°
- Angle is decreased if distal radius is dorsally angulated or the volar rim rotates dorsally
- Best assessed on 10° lateral view
- Volar tilt
- Normal ~11°
- AP width of the distal radius
- Normal ~19mm

What are the criteria for surgical treatment of distal radius?
- AAOS clinical practice guideline [J Am Acad Orthop Surg 2010;18: 180-189]
- Radial shortening >3 mm
- Dorsal tilt >10°
- Intra-articular displacement or step-off >2mm
- AAOS comprehensive review [AAOS comprehensive review 2, 2014]
- Loss of reduction
- Ulnar variance >5mm positive
- Dorsal angulation ≥15°
- Loss of radial inclination >10°
- Articular gap or step off ≥2mm
- Unstable Smith fractures
- Volar Barton shear fractures
- Open fracture
- Fractures associated with neurovascular injuries
- Fractures associated with intercarpal ligament injuries
- Polytrauma (relative)
3. Rockwood and Green [Rockwood and Green 8th ed. 2015] - Positive ulnar variance >3mm
- Carpal malalignment
- Dorsal tilt >10 if carpus aligned
- Neutral if carpus malaligned
- Articular gap or step >2mm
What are the surgical options for management of distal radius fractures?
[Rockwood and Green 8th ed. 2015]
- CRPP
- Options:
- Pins across fracture
- Pins from radius to ulna
- Intrafocal pins (Kapandji technique)
- ORIF with volar plating
- ORIF with dorsal plating
- External fixation
* Bridging ex-fix with pins in 2nd metacarpal and radius at distal 1/3-2/3 junction- 3mm pins in 2nd MC at base
- 4mm pins in radius between BR and ECRL
- Nerves at risk with radius pins = superficial radial nerve and LABC
* Nonbridging with pins in the distal fragment and radius at distal 1/3-2/3 junction
* +/- augmentation with percutaneous pinning, limited ORIF, bone graft or substitute
- Distraction bridge plating [JAAOS 2017;25:77-88]
- 2 incisions
- Over 2nd metacarpal and proximal to outcroppers
- Plate is passed deep to outcroppers and superficial to the ECRB and ECRL
- Plate is fixed to 2nd metacarpal and radial shaft

What are complications of CRPP for distal radius fractures?
[Rockwood and Green 8th ed. 2015]
- Superficial radial nerve injury
- Pin track infection
What are complications of bridging ex-fix for distal radius fractures?
[Rockwood and Green 8th ed. 2015]
- Pin track infection
- Loss of reduction/malunion
- Hand stiffness
- Superficial radial nerve injury
What are complications of nonbridging ex-fix for distal radius fractures?
[Rockwood and Green 8th ed. 2015]
- Overreduction
- Tendon injury
What are complications of volar locked plating for distal radius fractures?
[Rockwood and Green 8th ed. 2015]
- Screw penetration into DRUJ or radiocarpal joint
- Avoid intraoperatively by:
- Assessing tilted lateral view
- Radius is inclined 22 degrees off the table
- Assessing oblique views
- Examining flexion/extension at end of procedure
- Assessing tilted lateral view
- Tendon injury
- EPL rupture due to screw prominence dorsally
- Avoid by reducing measured length of screw by 2mm
- Dorsal horizon view
- Wrist is hyperflexed and the beam of the fluoroscopy unit is aimed along the longitudinal axis of the radius [J Hand Surg 2011;36A:1691–1693]
- Radial groove view
- Wrist is flexed almost fully, and the angle between the longitudinal axis of the forearm and the beam was 20° in the horizontal plane (forearm taken ulnar) and 5° in the sagittal plane (forearm taken dorsal)
- FPL rupture due to plate prominence
- Avoid by ensuring distal end of plate is proximal to watershed line – highest/most prominent point of the volar distal radius

What are the 3 columns of the wrist?
[JAAOS 2017;25:77-88]
- Radial column
- Consists of the radial styloid and scaphoid fossa
- Attachments
- Brachioradialis
- Long radiolunate ligament
- Radioscaphocapitate ligament
- Function
- Buttress to radial carpal translation
- Load bearing with the wrist in ulnar deviation
- Holds carpus out to length allowing more uniform distribution of load across the scaphoid and lunate facets
- Anchors the radioscaphocapitate ligament which prevents ulnar translation of the carpus
- Fracture
- Single large fragment from interfossal ridge to the metadiaphysis
- Intermediate column
- Fracture results in 4 fragments
- Volar rim
- Palmar instability if volar Barton pattern
- Axial instability (dorsal carpal translation) if dorsiflexion/impaction pattern
- Associated with DUC, dorsal wall +/- free intra-articular fragment
- Dorsal ulnar corner (DUC)
- May result in articular incongruity of DRUJ
- Dorsal wall
- Provides stability against dorsal subluxation
- Free intra-articular fragments
- Volar rim
- Volar rim and DUC
- Form most of the lunate facet and sigmoid notch
- Attachments
- Volar rim
- Short radiolunate ligament
- Volar radioulnar ligament
- DUC
- Dorsal radioulnar ligament
- Dorsal wall
- Dorsal radiocarpal ligament
3. Ulnar column
- Dorsal radiocarpal ligament
- Volar rim
- Consists of the distal ulna and TFCC
- Role in DRUJ stability and forearm motion
- Pedestal
- Consists of the metadiaphysis of the distal radius
- Function:
- Supports the radial and intermediate column

When considering fragment specific fixation in a distal radius fracture, what is the order of fixation?
[JAAOS 2017;25:77-88]
Intermediate > radial > ulnar
- Intermediate = volar rim > DUC > free intra-articular fragment > dorsal wall

Following distal radius fracture ORIF what should be checked?
- All screws are extra-articular
- Radial inclined lateral view (radiocarpal joint)
- AP view (DRUJ)
- ROM for crepitation
- Screws are appropriate length
- Lateral view
- Dorsal horizon view
- Radial groove view
- Plate position
- Proximal to watershed line
- Centred on shaft on AP
- Articular reduction
- No intra-articular step or gap
- Teardrop angle restored to normal
- DRUJ stability
* Stress in neutral, pronation and supination - Missed injury
- Scaphoid, ulna, carpal fracture
- SL, LT, perilunate
What are the radiographic goals to be achived in the reconstruction of distal radius fractures?
[JAAOS 2017;25:77-88]
Radial shortening <5 mm
Radial inclination >15o
Radiocarpal intra-articular step-off/gap <2 mm
Sigmoid notch incongruity <2 mm
Tilt between 15o dorsal and 20o volar
What are anatomic features of the scaphoid?
- Articulates with:
- Scaphoid fossa of the radius
- Lunate
- Capitate
- Trapezium
- Trapezoid
- 80% of its surface is covered in cartilage
- Sections include:
- Proximal pole
- Distal pole
- Waist
- Tubercle
- Ventrolateral aspect of distal pole
- Capitate fossa
- Lunate fossa

What is the vascular supply to the scaphoid?
[Rockwood and Green 8th ed. 2015]
- Dorsal scaphoid branch of the radial artery
* Supplies proximal 80% via retrograde flow - Volar scaphoid branch of the radial artery
* Supplies distal 20%

What are indications for ORIF of the scaphoid?
[Rockwood and Green 8th ed. 2015]
- Proximal pole fractures
- Displacement >1mm
- Humpback deformity
- Measurements on sagittal CT
- Lateral intrascaphoid angle >35°
- Normal = 30+/-5°
- Dorsal cortical angle > 160°
- Normal = 140°
- Height-to-length ratio >0.65
- Normal = 0.6
- Lateral intrascaphoid angle >35°
- DISI
- Radiolunate angle >15 degrees
- Capitolunate angle >15 degrees
- Scapholunate angle >60 degrees
- Associated perilunate dislocation
- Associated distal radius fracture
- Comminuted fracture
- Unstable vertical or oblique fractures
- Delayed presentation

What are the radiographic views of the scaphoid?
[Tornetta]
- PA view
* Allows visualization of the proximal pole of the scaphoid - Semipronated oblique view
* Provides the best visualization of the waist and distal pole regions - Semisupinated oblique view
* Provides the best visualization of the dorsal ridge - Lateral view
* Permits an assessment of fracture angulation, carpal alignment, and carpal instability - PA view with the wrist in ulnar deviation
* Results in scaphoid extension, allowing visualization of the scaphoid in profile
What are the advantages of surgical fixation of nondisplaced or minimally displaced scaphoid fractures?
[JAAOS 2013;21:548-557]
- Earlier union [J Hand Surg Am. 2016;41(12):1135e1144]
- Surgery = 7.1 weeks
- Nonop = 11.4 weeks
- Avoids prolonged immobilization
- Allows earlier return to activity/work [J Hand Surg Am. 2016;41(12):1135e1144]
- Surgery = 6 weeks
- Nonop = 11 weeks
- No difference in rate of union
What is the preferred nonoperative treatment of scaphoid fractures?
[JBJS REVIEWS 2016;4(9):e3]
- Long arm or short arm cast including or not including the thumb leads to equivalent outcomes in the treatment of scaphoid fractures with immobilization
- Duration ~8-12 weeks
- Dependent on clinical and radiographic union
- When CT is used to assess union, immobilization is discontinued when >50% union achieved
What are the indications and advantages of the volar approach in scaphoid fractures?
[JAAOS 2012;20:48-57]
Indications:
- Distal pole and waist fractures
- Humpback deformity
Advantage:
- Preserves dorsal blood supply
Describe the volar approach to the scaphoid?
[JAAOS 2012;20:48-57]
- Interval between the FCR and radial artery
- Skin incision can be zig-zag, L-shaped, or at the glabrous/nonglaborus skin border (Wagner)
* Proximally parallel to FCR
* Distally parallel to the radial aspect of the thenar eminence
* “Standard Russe incision is made along the course of the flexor carpi radialis (FCR) tendon and extending distally along the border of the glabrous skin of the thenar eminence”* - The volar FCR sheath is opened and FCR retracted ulnar
- Radial artery is retracted radial
* Superficial palmar artery crosses the surgical field and may need ligating - Floor of the FCR sheath and capsule are incised inline with scaphoid to expose the distal 2/3
* Radioscaphocapitate and long radiolunate ligaments are incised
What is often required to obtain the start point for the guidewire during volar approach to the scaphoid?
Resecting proximal palmer portion of trapezium
What is the fixation construct for scaphoid ORIF?
[Tornetta]
Cannulated headless compression screw
- Use the larger Acutrak 2 screw when feasible
- Mini-Acutrak 2 system may be necessary if:
- Small scaphoid
- Fracture is located proximally such that insertion of an Acutrak 2 screw may result in inadvertent propagation of the fracture to the insertion site with fragmentation of the proximal scaphoid
- Mini-Acutrak 2 system may be necessary if:
What is the appropriate length of screw (measurement) for scaphoid ORIF?
[Tornetta]
Subtract 4mm from measured length (or more if compression is to be obtained)
What are the indications for a dorsal approach to the scaphoid?
Proximal pole fractures
Describe the dorsal approach to the scaphoid?
- 2-3cm Longitudinal incision from proximal Lister’s tubercle extending distal inline with 3rd metacarpal
- Skin flaps are raised over the extensor retinaculum
- Extensor retinaculum is incised longitudinally distal to Lister’s along with the dorsal hand fascia
- EPL, ECRB and ECRL are retracted radially, EDC is retracted ulnarly
- Radiocarpal T- capsulotomy is performed
- Transverse limb parallel to the distal radius proximally, longitudinal limb extending directly over the SL ligament
- Capsular flaps are elevated off the SL ligament and scaphoid
- Avoid disruption of SL ligament and dorsal scaphoid ridge
What is the start point of the guidewire for the dorsal approach to the scaphoid?
[Tornetta]
Membranous portion of the scapholunate ligament origin
What are the 3 radiographic views obtained when determining guidewire placement in scaphoid ORIF?
- PA
- Lateral
- 30° pronated lateral view
****Wire is placed along central axis
What is DISI (dorsal intercalated segment instability)?
- Fixed extension of the lunate >10 degrees
- Associated with:
- Scapholunate ligament disruption
- Displaced scaphoid fracture
What is VISI (volar intercalated segment instability)?
- Fixed flexion of the lunate
- Associated with:
* Lunotriquetral ligament disruption
What is the mechanism of injury of perilunate and lunate dislocations?
[Hand Clin 31 (2015) 399–408]
- Hyperextension
- Ulnar deviation
- Intercarpal supination
What is the Herzberg classification for perilunate/lunate dislocation?
[J Am Acad Orthop Surg 2011;19: 554-562]
Stage I = perilunate dislocation
- Dorsal dislocation of the capitate with respect to the lunate while the lunate remains in its normal position in the lunate fossa.
Stage II = lunate dislocation
- The capitate has reduced from its dorsally dislocated position to become colinear with the radius, dislocating the lunate into the carpal tunnel
- Stage IIA
- Lunate has subluxated out of its fossa but has rotated <90°
- Stage IIB - lunate rotation >90°

What is the sequence of injury propagation in perilunate/lunate dislocation?
[J Am Acad Orthop Surg 2011;19: 554-562]
Disruption of scapholunate ligament → disruption of space of Poirier (capitolunate articulation) → disruption of the lunotriquetral ligament → disruption of dorsal radiocarpal ligament

What is the space of Porier?
[Rockwood and Green 8th ed. 2015]
Area of capsular weakness over the capitolunate articulation between the radioscaphocapitate and radioscopholunate ligaments

What is the Mayfield classification?
[Clin Orthop Relat Res. 2012 Apr; 470(4): 1243–1245] [Hand Clin 31 (2015) 399–408]
Describes the progressive ligamentous injury around the wrist in 4 stages
- Stage I
- Disruption of the SL and radioscaphocapitate ligaments
- Stage II
- Disruption of the lunocapitate association
- Stage III
- Disruption of the LT ligament (perilunate dislocation)
- Stage IV
- Lunate dislocation

What is a greater arc vs. a lesser arc injury (wrist)?
[J Am Acad Orthop Surg 2011;19: 554-562]
- Greater arc injury = associated fracture of radial styloid, scaphoid, capitate, lunate, triquetrum, hamate
* In naming greater arc injuries, the prefix trans- is used before the name of the fractured bone - Lesser arc injury = purely ligamentous injury

What are the radiographic features of perilunate and lunate dislocations?
[J Am Acad Orthop Surg 2011;19: 554-562]
- PA radiograph
- Intercarpal gap
- Disruption of Gilula carpal arcs
- Loss of carpal height with overlapping of carpal bones (particularly capitate and lunate)
- Carpal-height ratio = carpal height/length of 3rd metacarpal
- Abnormal = <45% (normal 45-60%)
- Scapholunate ligament disruption
- Signet ring sign
2. Lateral view - Hallmark is loss of colinearity of the radius, lunate and capitate
- ‘Spilled tea-cup sign’ in lunate dislocation
What is the management of perilunate and lunate dislocation?
[J Am Acad Orthop Surg 2011;19: 554-562]
- Immediate closed reduction (Except for IIB)
- Perilunate reduction maneouvre
- Fingertraps with elbow at 90 and 10 pounds of traction for 10 mins
- First extend the wrist then apply traction then wrist flexion, should feel palpable clunk
- Lunate dislocation [IIA only]
- First wrist flexion then dorsally directed force applied to lunate to reduce it
- Then extend the wrist followed again by traction and wrist flexion while maintaining dorsal directed pressure to lunate
- Do not attemtp reduction of IIB lunate dislocation because ineffective and could damage the short radiolunate ligament and its vascular
contribution
- Surgical intervention in 3-4 days after swelling subsides
- In greater arc injuries fix the fractures prior to the ligaments
- Repair ligaments
- Consider suture anchors
- Protect repair with intercarpal K-wire or temporary screw fixation
- Consider carpal tunnel release if symptoms present
What are indications for a volar approach in context of perilunate/lunate dislocation?
[Hand Clin 31 (2015) 399–408]
- Lunate dislocation requiring open reduction
- Carpal tunnel release
Describe the volar approach to the wrist for lunate reduction?
[Hand Clin 31 (2015) 399–408]
- Longitudinal starting 3cm proximal to wrist ulnar to the palmaris longus
* Angled ulnarly across the wrist then extended inline with the ring finger - Transverse carpal ligament is incised
- Flexor tendons and median nerve are retracted laterally to expose the lunate
- The lunate is reduced by direct pressure and lunate reduction maneuver
- Volar capsule and ligaments repaired to maintain reduction
- Proceed to dorsal approach
What is the importance of the dorsal approach to the wrist in perilunate/lunate dislocation?
[Hand Clin 31 (2015) 399–408]
- Allows anatomic reduction of the carpal bones
- SL ligament repaired from dorsal
Describe the dorsal approach to the wrist for perilunate dislocation management?
[Hand Clin 31 (2015) 399–408]
- Longitudinal incision centered over Lister’s tubercle
- Extensor retinaculum is divided in line with the 3rd dorsal compartment and EPL is retracted radially
- The 2nd and 4th compartments are elevated off the dorsal capsule
- A longitudinal or ligament-sparing capsulotomy (along DIC and DRC ligs) is made
Describe the carpal reduction, pinning and ligament repair for perilunate dislocation?
[Hand Clin 31 (2015) 399–408]
- K-wires are placed in the scaphoid and lunate and used as joysticks
* K-wires are placed 45 degrees from vertical from distal to proximal in scaphoid and proximal to distal in lunate
* The pins are then made colinear and compressed together to reduce the SL interval - Once reduced, reduction is maintained by percutaneous pinning
* Pins include LT, SL, SC, TH - SL ligament repair follows reduction and K-wire stabilization
* Usually with suture anchor - Capsulotomy is repaired anatomically and dorsal ligaments are repaired
- Extensor retinaculum is repaired

What is the postoperative protocol after fixation of perilunate/lunate dislocation?
[Hand Clin 31 (2015) 399–408]
K wire removal at 10 weeks and therapy initiated
What is the management of a chronic perilunate dislocation?
[Hand Clin 31 (2015) 399–408]
- <3 months may still attempt open reduction
- >3 months will require salvage procedure
- Proximal row carpectomy
- Wrist arthrodesis if degeneration present
