SM_192b: Puberty Flashcards
Puberty is ___
Puberty is maturation of the hypothalamic-pituitary-gonadal axis

Describe biochemical changes of puberty
Biochemical changes of puberty
- Increase in pulsatile GnRH secretion (hypothalamus): increased frequency and amplitude, initially at night
- Increase in pulsatile LH and FSH (pituitary): increased frequency and amplitude, initially at night, diurnal rhythm lost as puberty progresses
- Increase in estradiol or testosterone (gonad: gonadarche)
Describe puberty over the lifespan
Puberty over lifespan
- Pubertal hormones: high in fetus, low in infant, especially low in child, then increases to high in adult
- CNS inhibition of GnRH pulse generator: low in fetus, higher in infant, highest in child, then decreases
Regulation of pubertal onset involves ____ and ____
Regulation of pubertal onset involves reactivation and stimulation / release of inhibition
Regulation of onset of puberty involves excitatory and inhibitory effects on ____ secretion
Regulation of onset of puberty involves excitatory and inhibitory effects on GnRH secretion
____ and ____ are the gatekeepers of puberty
Kisspeptin and neurokinin B are the gatekeepers of puberty

Kisspeptin levels ___ at pubertal onset
Kisspeptin levels increase at pubertal onset
- Administration of kisspeptin advances timing of puberty in rats

KISS1R knockout mice have ____ GnRH neurons but ____ and ____
KISS1R knockout mice have normal GnRH neurons but gonadotropin deficiency and no puberty (hypogonadotropic hypogonadism)

KISS1 protein activates ___
KISS1 protein activates GPR54/KISS1R

TAC3 encodes ____
TAC3 encodes TACR3 / NKB receptor

____ acts upstream to release of kisspeptin, so mutations lead to ____ then ____
Neurokinin B acts upstream to release of kisspeptin, so mutations lead to hypogonadism than reversal in adulthood
(important for puberty, not reproduction)

____, ____, ____, and ____ are regulators / modulators of the hypothalamic-pituitary-gonadal axis
Gonadal steroids (T or E), metabolic hormones (leptin, ghrelin), sleep, and overall energy balance are regulators / modulators of the hypothalamic-pituitary-gonadal axis

Anorexia nervosa involves ____
Anorexia nervosa involves inadequate energy balance that suppresses production of GnRH, LH, and FSH

___ is important in the development / function of GnRH producing neurons
KAL1 / ANOS1 is important in the development / function of GnRH producing neurons
Excitatory regulation of onset of puberty occurs via ____, ____, ____, and ____
Excitatory regulation of onset of puberty occurs via leptin, KISS1 / GPR54, neurokinin B, and adequate energy balance
(KAL1 / ANOS1 -> development / function of GnRH-producing neurons)

Inhibitory regulation of onset of puberty occurs via ____, ____, and ____
Inhibitory regulation of onset of puberty occurs via GABA, beta endorphin, and MRKN3
(KAL1 / ANOS1 -> development / function of GnRH-producing neurons)

Describe puberty (gonadarche)
Puberty (gonadarche)
- Sexual maturation
- Reproductive capability
- More accurately described as gonadarche
- Maturation of hypothalamic / pituitary / gonadal axis
- Inbcrease in GnRH, LH, FSH, and testosterone or estrogen / estradiol
Adrenarche is ____
Adrenarche is maturation of the hypothalamic-pituitary-adrenal axis
- Andrenal androgens increase (DHE, DHEA-S, androstenedione)
- Independent of puberty
Puberty (gonadarche) and adrenarche are ___ but ___
Puberty (gonadarche) and adrenarche are temporally related but independent
Describe adrenarche, pubarche, gonadarche, and menarche
- Adrenarche: adrenal maturation
- Pubarche: presence of pubic hair
- Gonadarche: onset of gonadal maturation (true puberty)
- Menarche (onset of menses)
Describe pubertal labs
Pubertal labs
- LH: 0.3-15 mIU / mL
- FSH: 0.8-11 mIU / mL
- Estradiol: 16-300 pg / mL
- Testosterone: 10-1000 ng / dL
- DHEA-S: 90-300 mcg/dL
First sign of central puberty (gonadarche) in girls is ____
First sign of central puberty (gonadarche) in girls is breast development (thelarche)

First sign of central puberty (gonadarche) in boys is ____
First sign of central puberty (gonadarche) in boys is testicular enlargement

___ promote pubic hair, axillary hair, body odor, and acne in puberty
Androgens promote pubic hair, axillary hair, body odor, and acne in puberty
- Predominantly adrenal androgens, particularly in girls
- Some from gonadal testosterone in boys
- Presence of pubic hair is called pubarche (not adrenarche unless DHEA-S is elevated into adrenarche range)
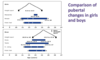
Describe puberty in girls
Puberty in girls
- Average pubertal onset: 10 years
- Range of normal: 8-13 years old
- Menarche average: 12.5 years
- Peak growth rate: Tanner 2-3
- Menarche: Tanner 4 breast development

Describe puberty in boys
Puberty in boys
- Average pubertal onset: 11.5 years
- Range of normal onset: 9-15 years
- Gynecomastia: Tanner 2-3
- Voice change: Tanner 3-4
- Peak growth rate: Tanner 4
- Spermarche: Tanner 3-4
- Facial hair: Tanner 4-5

Puberty starts ____ in boys than girls
Puberty starts later in boys than girls
Variations of normal puberty are ____, ____, ____, and ____
Variations of normal puberty are premature thelarche, premature, pubarche, premature adrenarche, and constitutional delay of puberty
Precocious puberty is ____ in girls and ____ in boys
Precocious puberty is < 8 years in girls and < 9 years in boys
Delayed puberty is ____ in girls and ____ in boys
Delayed puberty is > 13 years in girls and > 15 years in boys
(delayed puberty is also defined by an elapsed time of > 4 years from the onset of puberty to menarche or full testicular development)
Describe evaluation of puberty
Evaluation of puberty
- History: congenital anomalies, other endocrine or medical problems
- Family history of pubertal onset
- Physical examination
- Bone age
- Laboratory evaluation ± provacative testing
- Imaging: MRI of pituitary and hypothalamus, ultrasound / MRI / CT of gonads / pelvis / adrenal glands as indicated
Central precocious puberty is ____, involving ____ and ____
Central precocious puberty is GnRH dependent, involving pubertal LH / FSH and testosterone or estradiol
- Idiopathic
- CNS abnormalities: acquired, congenital, tumors, chronic exposure to sex steroids
Peripheral precocious puberty is ____, involving ____ and ____
Peripheral precocious puberty is GnRH independent, involving low/prepubertal LH / FSH and pubertal / high testosterone or estradiol
- Genetic (LH receptor activating mutations, McCune Albright syndrome)
- Tumors
- Other
____ is a common cause of peripheral precocious puberty
McCune Albright syndrome is a common cause of peripheral precocious puberty
Peripheral precocious puberty is GnRH independent, involving low/prepubertal LH / FSH and pubertal / high testosterone or estradiol
McCune Albright syndrome classic triad is ____, ____, and ____
McCune Albright syndrome classic triad is peripheral precocious puberty, cafe au lait spots, and polyostotic fibrous dysplasia
- Peripheral precocious puberty: episodic ovarian cysts in girls
- Polyostotic fibrous dysplasia: bone dysplasia
- Can have hyperfunction of other hormones: TSH, GH, ACTH
Gonadotropin levels will be ____ in central precocious puberty
Gonadotropin levels will be pubertal in central precocious puberty
Sex steroid levels are ___ in central precocious puberty
Sex steroid levels are pubertal in central precocious puberty
Gonadotropin levels are ____ in peripheral precocious puberty
Gonadotropin levels are prepubertal in peripheral precocious puberty
Sex steroid levels are ____ in peripheral precocious puberty
Sex steroid levels are pubertal in peripheral precocious puberty
Central precocious puberty has pubertal levels of ____ and ____
Central precocious puberty has pubertal levels of gonadotropins and sex steroids
Peripheral precocious puberty involves prepubertal (low levels) of ____ but pubertal ____
Peripheral precocious puberty involves prepubertal (low levels) of gonadotropins but pubertal sex steroids
Delayed puberty may be caused by ____
Delayed puberty may be caused by hypogonadotropic hypogonadism
Hypogonadotropic involves the ____, ____, and ____ and causes ____ and ____
Hypogonadotropic involves the central, hypothalamic, and pituitary, and causes low / prepubertal LH / FSH and low testosterone or estradiol
____ is a common cause of hypogonadotropic hypogonadism
Kallmann syndrome is a common cause of hypogonadotropic hypogonadism
Describe Kallmann syndrome
Kallmann syndrome
- Hypogonadotropic hypogonadism due to failure of the GnRH neuron and olfactory placode migration
- X-linked most commonly caused by mutations in KAL1 (ANOS1) gene
- Can also be autosomal dominant
- Anosmia
- Other possible findings: coloboma, synkinesis (mirror image movements), hearign loss, single kidney
Delayed puberty may be caused by ____
Delayed puberty may be caused by hypergonadotropic hypogonadism
Hypergonadotropic is ____ and involves ____ and ____
Hypergonadotropic is primary / gonadal and involves very high LH / FSH and low testosterone or estradiol
- Acquired
- Congenital
A 16 year old girl had thelarche at 11 years old but has not had menarche yet. Is this delayed puberty?
A 16 year old girl had thelarche at 11 years old but has not had menarche yet. Is this delayed puberty?
Yes
A 16 year old boy has 2 mL testes, Tanner 1 pubic hair, no voice change and no body odor. Is this delayed puberty?
What diagnoses are on your differential?
A 16 year old boy has 2 mL testes, Tanner 1 pubic hair, no voice change and no body odor. Is this delayed puberty?
Yes
What diagnoses are on your differential?
Hypogonadotropic hypogonadism: Kallmann syndrome, optic nerve hypoplasia, chronic illness, tumor, h/o radiation treatment, malnutrition, elevated prolactin or cortisol
If LH and FSH are very high and testosterone, what diagnoses are on your differential?
If LH and FSH are very high and testosterone, what diagnoses are on your differential?
- Cognenital: Klinefelter syndrome, gonadal dysgenesis
- Anatomic: anorchia, bilateral testicular torsion
- Acquired: chemotherapy, radiation treatment, infectious (mumps)
