Slide Exam Cards from Quizlet Flashcards
(89 cards)
.Name, define, causes (2), features (5), biopsy (2)

Conjunctival Papilloma: (def: overgrowth of epithelial cells)
- Cause: Excess UV or HPV infection (HPV in 39% of cases)
- Features: non-malignant, motile, doesn’t involve cornea, modest feeder vessels, pinkish (less red),
- Biopsy: BM still intact, non-invasive of stroma
.Name, causes (2), features (5), biopsy (2)

CIN (conjunctival intraepithelial neoplasia:
Cause: Excess UV or HPV (in 39%)
Features: Non-malignant, motile, more marked BV strawberry spots, more lush feeder vessels, invades corneal epithelium (but NOT stroma or substantia propria)
Biopsy: Non-invasive of stroma, plemorphism and metaplasia present
Name, features/biopsy (4), DDx

SCN:
Features/biopsy: malignant, non-motile, broken through basement membrane and invading stroma/substantia propria, may see ulceration (with white plaques) and small haemorrhages
DDx: requires OCT or biopsy, b/c CIN-like appearance
(note: non-motile as anchored by stromal invasion)
Name each condition and compare: Redness, Feeders, Corneal invasion, Stromal invasion (OCT), Motile (OCT), Malignancy, Pleomorphic, Surgery

Papilloma: redness (+), feeders (+), corneal invasion (-), stromal invasion (-), motile (+++), malignancy (-), pleomorphic (-), surgical removal (optional)
CIN: redness (+++), feeders (+++), corneal invasion (++), stromal invasion (-), motile (++), malignancy (+), pleomorphic (++), surgical removal (YES)
SCN: redness (+++), feeders (++++), corneal invasion (++++), stromal invasion (++++), motile (-), malignancy (++++), pleomorphic (++++), surgical removal (YES)
.Name, define, features (6)

Naevus: Benign ocular pigmented lesion
Usually forms in 10-20YO.; Slow growing; 1% become malignant.; Flat or minor elevation.; Colour varies, commonly 1-2 feeder vessels
Name, features (3), Dx (3), Mx (1)

Congenital melanocytosis
.- Pigment in sclera- 2-4% get malignancy.- Not Motile (no conj.)- - -
Dx: F.A.T, annual photos, DFE for choroidal melanoma
Mx: (if malignant) refer for excision + biopsy
Name, characteristics (5)

Primary Acquired Melanosis (PAM):
.- Older + middle aged + fair skinned at risk.- Diffuse brown colour + acquired.- Unilateral.- Flat + Mobile over sclera.- Concerns for melanoma-
Name, features (6)

Melanoma
- 75% come from PAM.- invasive.- Fast growth.- Dense Colour (may be Diffuse at edge).- Irregular boundary.- Feeders
Name, describe appearance, is it symptomatic?

Telangiectasia:
.- Corkscrew squiggly or masses of BV- Asymptomatic, cosmetic or systemic disease indicator- - - -
Name, define/features (3)
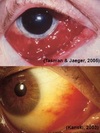
Kaposi’s sarcoma:
.- malignant tumor (overgrowth) of the blood vessels associated with AIDS (immunocompromised)- - bright red vascular mass - most often inferior fornix- -
Name, characteristics (3).

Sturge-Weber Syndrome
.- Effects seen along trigeminal nerve- Episcleral/conj involvement in 70%.- Congenital conjunctival or Episcleral haemangioma
.Name, define, mx (1)

Cavernous sinus fistula:
.- Break in the cavernous sinus- i.e. “fistula” = break in wall of an artery –> causing higher arterial blood to enter venous space—-
Mx: refer for closure of fistula + mx of IOP
.Name, features (3)

Cyst of Moll/sweat glands
- Clear, fluid, translucent balloon; - syringoma (multiple+flat); - milia (multiple hard pimples)
Name, describe (2)

Cyst of Zeis Gland - Opaque lesion
- Visible lesion at lash root, often hair follicle, Appears slight yellow/white and opaque/milky (not translucent like Moll)
Name, describe (1), causes (2), a symptom (1)

Stye/Hordeolum
.- Blockage of duct.- due to bacterial infection (external) or complication of chalazion (internal)- discomfort
Name, describe, symptoms (3)

Chalazion
.- Blockage of MG.- Inflammation- symptoms: cosmesis, generally painless, does not affect V.A (only lower lid)
Name, describe (5)

Sebaceous gland carcinoma
.- elderly females (chronic bleph)-yellow and hard - madarosis with thickened, red lid margins (UL) - >2mm 60% mortality—
Name, cause (1), describe (2)

Viral Warts (Verruca)
.- Viral Infection from HPV.- Papule or elongated filliform—-
Name, cause (1), describe (1)

Molluscum contagiosum
.- Viral Infection from pox virus- Flatter dome-shaped lesion (1-3mm)—-
name, describe (3)

Keratoacanthoma
- Benign neoplasm, mimics squamous cell carcinoma, resolves spontaneously- - —
Name, describe (1)

Xanthelasma
- soft, raised yellow plaques occurring on the skin at the inner corners of the eyes—–
Name, describe

Seborrheic Keratosis (SK):
- A superficial benign neoplasm of epidermal cells that presents as a papule or plaque with a characteristic “stuck-on” appearance. These lesions are usually acquired later in life and tend to grow slowly.- - —
Solar or Actinic Keratosis (3)
.- Scaly apperance.- Benign skin tumour.- Just cosmetically unappealing—

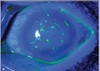
Epithelial Basement Membrane Dystrophy (EBMD): what is it also known as? how common is it? describe it’s appearance
.- Also known as map-dot fingerprint dystrophy.- Most common corneal dystrophy but often misdiagnosed due to variable appearance—-