S4) Lipid Transport Flashcards
Lipids are a structurally diverse group of compounds.
Categorise lipids

Lipids are hydrophobic molecules, hence insoluble in water.
How are they transported in light of this?
Lipids are transported in blood bound to carriers
How are different types of lipids transported in the blood?
- ~ 2% of lipids (fatty acids) are carried bound to albumin (limited capacity)
- ~ 98% of lipids are carried as lipoprotein particles consisting of phospholipid, cholesterol, cholesterol esters, proteins & TAG
Describe the structure of a phospholipid molecule

Where are phospholipid molecules seen?

Describe the formation and function of cholesterol
- Formation: some obtained from diet, but most synthesised in liver
- Function: essential component of membranes (modulates fluidity)
Cholesterol also acts as a precursor for several molecules.
Identify some
- Precursor of steroid hormones e.g. cortisol, aldosterone, testosterone
- Precursor of bile acids
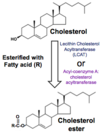
How is cholesterol transported?
Transported around body as cholesterol ester
Describe the structure of a lipoprotein molecule

What are the contents of a lipoprotein molecule?

What are the two types of apolipoproteins found on a lipoprotein molecule?

There are five distinct classes of lipoproteins named according to density.
Identify them
- Chylomicrons
- VLDL (very low density lipoproteins)
- IDL (intermediate density lipoproteins)
- LDL (low density lipoproteins)
- HDL (high density lipoproteins)
Illustrate how each type of lipoprotein contains variable content of apolipoprotein, triglyceride, cholesterol and cholesterol ester

Lipoprotein density is obtained by flotation ultracentrifugation.
What is the observed relationship between density and diameter?
Particle diameter is inversely proportional to density

Rank the different lipoprotein molecules according to their density and diameter

What is the relationship between lipoproteins and apolipoproteins?
Each class of lipoprotein particle has a particular complement of associated proteins (apolipoproteins)

Which two apolipoproteins are of clinical significance?
- apoB (VLDL, IDL, LDL)
- apoAI (HDL)

Identify the two roles of apolipoproteins
- Structural: packaging water insoluble lipid
- Functional: co-factor for enzymes and ligands for cell surface receptors
In 8 steps, outline chylomicron metabolism
⇒ In small intestine, apoB-48 added to chylomicrons before entering lymph
⇒ Travel to thoracic duct & empties into left subclavian vein
⇒ Acquire 2 new apoproteins (apoC and apoE) once in blood
⇒ apoC binds lipoprotein lipase on adipocytes and muscle
⇒ Released FA enter cells depleting fat content in chylomicron
⇒ Chylomicron remnants return to liver
⇒ LDL receptor on hepatocytes binds apoE, chylomicron remnant taken up by receptor mediated endocytosis
⇒ Lysosomes release remaining contents for metabolic use

Illustrate the relationship between VLDL, IDL and LDL metabolism

In four steps, describe how LDL enters peripheral cells by receptor mediated endocytosis
⇒ Cells requiring cholesterol express LDL receptors on plasma membrane
⇒ apoB-100 on LDL acts as a ligand for these receptors
⇒ Receptor/LDL complex taken into cell by endocytosis into endosomes
⇒ Fuse with lysosomes for digestion to release cholesterol and fatty acids

Illustrate a summary of HDL metabolism in terms of the following:
- Formation
- Maturation
- Reverse cholesterol transport
- Cholesterol transfer
- Breakdown

Identify and describe the three clinical signs of hypercholesterolaemia
- Xanthelasma – yellow patches on eyelids
- Tendon xanthoma – nodules on tendon
- Corneal arcus – obvious white circle around eye (common in older people)

Raised serum LDL is associated with atherosclerosis.
Outline the pathway in which oxidised LDL leads to angina, myocardial infarction or stroke due to atherosclerosis

Illustrate the different stages between plaque formation and plaque rupture

Describe the method of action of statin drugs in the pharmacological treatment of hyperlipoproteinaemias
