Physiology 1 22 Flashcards
There are two components to respiration what are they ?

The two compenents of respiration = Internal and External
External respiration = external environment to tissue
- Ventilation = bulk transport of external media across a gas exchange surface
- respiratory exchange - diffusion
- circulation
- cellular exchange
Internal respiration = cellular metabolism

What is Dalton’s law ?
Daltons law
- the partial pressue of gas
- the total pressure of a gas is equal to the sum of the partial pressures of the individual gases in a mixture
With altitude as the total pressure decreases, the partial pressure of a particular gas will decrease.
Partial pressure of oxygen = PO2
The partial pressure of any gas will change with environment.
What is Henry’s law ?
Henrys law
The amount of gas dissolved in a liquid is afftected by the gases partial pressure and solubility coefficient of that gas.
gas dissolved = pressure of gas in the media * solubility coefficient
- gas and liquid are in equilibrium
- only free gas molecules (physically dissolved contribute to the partial pressure of gas in liquid)
- gases will always diffuse down their partial pressure gradients.

What is Fick’s law, and what four factors affect the rate of diffusion ?
Describes the net diffusion rate of a gas across a fluid membrane.
- gases move down their partial pressure across a semi permeable membrane
Rate of diffusion
- surface area
- thickness or distance (T)
- pressure gradient (P)
- Diffusion coefficient (D)
What is Boyle’s law ?
Boyle’s law
For a fixed amount of an ideal gas kept at a fixed temperature, pressure and volume are inversly proportional.

What is tidal breathing and flow through breathing ?

Flow through breathing
- unidirectional flow of media, yeilds greater O2 uptake
- birds, fish and some crocodiles
Tidal breathing
- relatively inefficient as external medium moves in and out through the same opening
- mammals (bidirectional).
- fresh media is mixed with depleted media

Describe concurrent, cross current and countercurrent gas exchange ?
Concurrent exchange
- external medium and blood flows in the same direction
- partial pressure gradient declines
- does not exist in a biological system
Cross current exchange
- external medium and blood travels at right angles to each other
- diffusion occurs through-out declines gradually
- PO2 is higher in blood then external medium at the end
- birds
Coutercurrent exchange
- external medium and blood flows in the opposite direction and parallel to each other
- partial pressure gradient is maintained and diffusiin is constant
- fish highly efficient

Describe gas exchange in fish through the use of gills ?2
Gills
- countercurrent exchange system
- flow through
- at every point O2 is diffused into blood - great efficiency in gas exchange
- four gill arches - filaments - lamella
- large surface area which is proportional to how active the fish is
Buccal pressure pump - fish opens and closes mouth
Opercular suction pump - fish open and close opercular flaps

Describe the upper and lower respiratory tract, what are these systems purpose?

Upper respiratory tract
- located outside the chest cavity
- no gas exchange anatomical deadspace
- covered with mucus and ciliated epithelium
- trachea and bronchi supported by cartilage
- smooth muscle lines trachea, bronchi and bronchioles.
Function = conditioning of air (warm, humidification), and filtration muco-ciliary escalator
Lower respiratory tract
- alveolar surface thin layer of squamous epithelial cells (type one)
Contains three cell types
- Type one alveolar cell - assist in gas exchange
- Type two - large cuboidal produce surfactant
- Alveolar macrophage - phagocytic patrol the alveolar surface.

Hoe does air move into the lungs ?
By creating negative pressure. Increasing volume by contraction of the diaphragm and external intercostal muscles.
Describe the histological sections of the upper respiratory tract ?
Trachea = C shaped cartilage
Bronchi = cartiliginous plates
Bronchioles do not have cartilage
The amount of smooth muscle increase from the trachea to the bronchioles.

Describe the histology of the alveolar ?
Alveolar
- Alveolar surface covered by a dense capillary surface, lung interstitium has mast cells, connective tissue and elastic tissues to hold the alveolar open.
- mainly composed of type one alveolar cells - single layer of a single layer of sqaumous epithelial cells.
- Type two alveolar cells are cuboidal and secrete surfactant and the fluid layer which lines the lungs
- Alveolar macrophage

What effect does the parasympathetic and sympathetic nervous system have on the lungs ?
Sympathetic
- air way relaxation
- blood vessel constriction
- inhibition of glandular secretion through beta 2 receptors
Parasympathetic
- air way constriction
- blood vessel dilation
- increased glandular secretion
- vagus nerve

Describe the intrapleural space and the intrapleural pressure, and what they do?

Intrapleural space
- pleura anatomically seperates the lungs from the thoracic wall
- enables friction free movement between the lungs and the thorax
- lung is mechanically connected to the thoracic cage and pleura by the pleural fluid
- pressure of fluid is negative (intrathoracic pressure) holds the lungs open
- -3mmhg
- intrapleural space of the two lungs is seperated in most species
- cause for negativity is the mechanical interaction between the lungs and chest wall.
During quiet inspiration the intrapleural pressure becomes more negative, while during expiration it becomes less negative.

What is the intrapulmonary pressure (Palv) ?
Alveolar or intrapulmonary pressure is the pressure of the air inside the lung alveoli
Normal respiration alveolar pressure decreases to about -1 mmhg (inspiration) and rises to about 1mmhg during expiration.

What is the transpulmonary pressure ?
Transpulmonary pressure
Is the difference between the alveolar pressure and the pleural pressure (distending pressure)
- the more positive the distending pressure ptp becomes the more the lungs are distended or inflated
- ptp= Palv -Ppl

Describe Pulmonary ventilation in mammals ?
Inspiration
- diaphragm and intercostal muscles contract
- lung volume increases
- lung pressure decreases belwo atmospheric pressure
- air flows down its concentration gradient
- inspiration is always active as it requires muscle contraction
- 1-2% of the total energy metabolism
Expiration
- diaphragm and intercostal muscles recoil
- lung volume decreases
- lung pressure increases
- internal intercostal muscles may contract to assist with expiration
- passive process in rest

What is eupnea ?
normal quiet breathing
What is Hyperpnea ?
increased depth and frequency of breathing during exercise
What is Tachypnea ?
excessive rapidity of breathing
What is bradypnea ?
abnormal slowness of breathing
What is polypnea ?
rapid shallow breathing, as occurs during panting
What is dyspnea ?
Difficult, painful or laboured breathing - pathological
What is apnea ?
cessation of breathing, in clinic refers to transient state of cessation of breathing
What are adventitious sounds ?
crackles and wheezes abnormal sound superimposed on normal breath sounds.
Why do birds need a more efficient gas exchange system when compared to mammals ?
Birds are exothermic with a higher body temperature - 40-41 degrees
Highly active - flying high altitudes where the partial pressure of oxygen is lower.

How do birds achieve a greater efficiency in respiration when compared to humans ?
Greater efficiency of respiration in birds
- narrow diffusion distance air capillaries
- flow through breathing unidirectional
- cross current breathing

How does the bird’s respiration system work ?
Bird
- During inspriration both the anterior and posterior air sacs expand
- During expiration both the anterior and exterior air sacs deflate
- allows for flow through breathing
- lung relatively rigid and the air sacs act as bellows
- both inspiration and expiration are active even at rest
- respiratory muscles act upon the sternum to reduce or increase pressure within the air sacs
- air exchange occurs in the parabronchi ( air capillaries)
Requires two cycles to move a single bolus of air through the entire system.

What is lung compliance ?

Lung compliance is a measure of how much force is required to distend the lung.
- the greater the change in volume, with a smaller force = greater compliance
- lung and thoracic structures
- alveolar surface tension

Why is the surfactant produced by type two alveolar cells so crucial ?

Surfactant
Surface tension acts to reduce the surface area collapsing the alveolar.
Surfactant reduces surface tension .
- prevents alveolar from collapsing
- reduces effort to expand lungs
- prevenst adhesion of adjacent respiratory surfaces
Barker syndrome = in piglets and horses is caused by too low a production of surfactant during gestation. The animal requires excessive force to extend lungs and rapid expiration.

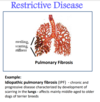
What is a restrictive disease of the lungs, provide an example and type of breathing pattern this will generally cause ?
Restrictive disease
- results in restriction of lung expansion
- pulmonary fibrosis - progressive scarring of the lungs seen in older terriers
- causes rapid shallow breathing
What is an obstructive lung disease, provide an example and what type of breathing pattern this will generally cause ?
Obstructive lung disease
- Causes obstruction within the airways - decreasing airway diameter
- decrease in airway diameter occurs during expiration (due to positive intrapleural pressure)
- expiratory dyspnoea
- animals abnormally slow and deep breathing pattern.
Examples
- Heaves in horses = hypersensitive to allergens
- Feline asthma inflammation and constriction of the bronchioles

In a spirogram we can obtain four lung volumes of TV, IRV, ERV and RV difine these volumes.
The four volumes obtained in a spirogram.

Tidal volume (TV or VT) = volume of air inhaled or exhaled per breath
Inspiratory reserve volume (IRV) = amount of additional air that can be taken into the lungs after a normal inspiration.
ERV = amount of additional air than can be taken from the lungs after a normal expiration.
Residual volume = amount of air remaining in the lungs after maximal expiration (can not be measured by spirometry).
Describe what will happen if lung compliance becomes abnormal ?

Higher than normal compliance
- Lung inflates easily but due to reduced elastic recoil it becomes difficult to expire
- emphysema
Lower than normal compliance
- Requires increased force to expand alveoli
- pulmonary fibrosis

Define the four lung capacites inspiratory capacity, functional residual volume, vital capacity and total lung capacity obtained in a spirogram ?
Four lung capacity
Inspiratory capacity = IRV + TV
Functional residual capacity = ERV + TV
Vital capacity = ERV + IRV + TV
Total lung capacity (TLC) = VC + RV
Define PEFR and PIFR ?
Peak flow rate can be taken as a quick measurement and is useful to monitor obstructive diseases.
PIFR = Peak inspiratory flow rate
The fastest flow rate achieved during inspiration
PEFR = Peak flow rate achieved with maximal force during expiration after a complete inspiration.
Define minute ventilation ?
Minute ventilation
Minute ventilation = The volume of air breathed in or out within one minute.
mV = RR * TV
- increases during physical activity
- gives the volume flow throughout the entire respiratory tract including lungs
Define respiratory dead space, anatomical dead space, and physiological dead space ?
Respiratory dead space = air that enters the lungs but dose not participate in gas exchange.

Anatomical dead space = air which fills conducting airways, conditioning, thermoregulation
Alveolar dead space = gases which enter the alveolar but do not participate in gas exchange eg no perfusion.
Physiological dead space = alveloar dead space + anatomical dead space
In a normal healthy lung the physiological dead space = anatomical dead space as a healthy lung has no alveoli dead space.
Define alveolar ventilation ?
Alveolar ventilation accounts for the fact that not all minute ventilation contributes to gas exchange
Alveoli ventilation = (TV - dead space volume) * RR
It is the rate at which the alveolar air is replaced by atmospheric air.
What is the Va / Q ration and why is it important in respiration ?a
For gas exchange to occur efficiently the ventilation of th lungs to perfusion ratio must be matched
Va / Q = 1 Maximum gas exchange
- If perfusion of the lungs increases the bronchioles, alveoli will dilate in response to increase ventilation: and vice versa
- local control mechanisms
- bronchiole dilates - arterioles dilate
- bronchiole constricts - arterioles constrict
Mismatching of the Va and Q are the main causes of hypoxemia

What happens during mismatching of ventalation and perfusion, and provide an example ?

Ventalation Va and perfusion Q mismatching occurs in abnormal conditions
- healthy perfusion ventilation ratio = 1
- as the degree of mismatching increases, O2 exchange becomes less efficient
- most common cause of hypoxemia decreased 02 in the blood
Eaxamples
- Shunt = blockage of the airway (mucous plug) so perfusion without ventilation
- embolism = blockage of an artiole ventilation without perfusion

Why would impairment of partial pressure gradient affect 02 but not CO2?
Diffusion coefficient is higher in CO2, than O2

Describe how O2, and CO2 are transported around the body and it what proportions ?
Blood needs to carry more gas than can dissolve in plasma.
Oxygen is carried in two forms
- bound to haemoglobin 98.5%
- unbound dissolved 1.5%
Carbon dioxide is carried in two forms
- carbaminohemoglobin (3) as bicarbonate form
Oxygen bound to hemoglobin dose not contribute to PO2
- this maintains oxygen gradient in the lung
- the amount of Hb in blood determines the oxygen carrying capacity of blood
- each HB molecule binds four O2 molecules when fully saturated

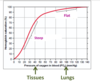
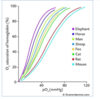
What shape is the hemoglobin oxygen disociation curve, why dose the flat part occur ?

The oxygen haemoglobin dissociation curve is sigmoid in shape.
The saturation of HB is related to the PO2 of the blood
The flat part
- Favors loading of oxygen and is due to a high PO2
- occurs in the lungs
- no significant change in % saturation between 60 - 100 mmHg
- at normal PO2 complete saturation of hemaglobin occurs
- large plateau of curve provides a large safety margin.
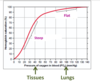
The sigmoid oxygen haemoglobin dissociation curve has a steep part why dose this occur.
Steep part
- curve shows steep decline in % saturation between 40 to 10 mmHg
- helps dissociate oxygen from the haemoglobin molecule
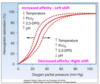
What four factors affect the affinity of Hb for O2, how would these facotors be changed to cause a decrease in affinity ?
The four factors
- temperature
- PH
- 2,3 DPG
- PO2
To cause a decrease in affinity
- temperature increases
- PH decreases
- 2,3 DPG increases
- PCO2 increases
What is the BOHr affect ?
An increase in carbon dioxide in the blood and a decrease in PH results in a reduction of the affinity of haemoglobin for O2.

What affect will exercise have on the oxygen - haemoglobin dissociation curve why dose this occur ?

Exercise
right shift of sigmoid curve decreased affinity - favoring unloading of oxygen to the tissues
note = at rest only 25% of oxygen bound to HB is released to the tissues in one circuit - so there is a large reserve of oxygen for increased metabolic rate.
Factors
- PO2 reduced metabolically active tissues / reduced saturation of HB 10-40mmHG
- CO2 increases in tissues
- acidity increases
- when tissues need more they get more

Dose the form of haemoglobin vary, and why would this occur ?
Haemoglobin form varies between species and life stages
Animals have varying form of Hb suited to their metabolic rate and environment
- small animals with fast metabolism have HB with low affinity - favoring oxygen unloading in tissues
- animals at high altitudes - HB higher affinity of for oxygen as the partial pressure of oxygen is lower
- The effect of CO2, H+ causes different affects on HB depending upon its form
- effect of 2,3 DPG varys depending on form
- Fetal HB often has a lower affinity for oxygen than in its adult form.
Describe the diffusion of oxygen at the tissue level ?
O2 diffusion tissue level
- Tissue PO2 at rest = 40 mmhg
- partial pressure of O2 systemic 100 mmhg
- partial pressure gradient = 60 mmhg
Oxygen diffuses from blood into the tissue down its partial pressure gradient.
Tissues with a higher demand for oxygen will be more highly vascularised.

Describe the diffusion of CO2 at tissue level ?

Tissue diffusion of PCO2
- tissue partial pressure = 45mmhg
- systemic blood partial pressure = 40mmhg
CO2 moves into blood from the tissues down its partial pressure gradient

Describe the three forms carbon dioxide is transported in, within the blood ?
- Bicarbonate 60%
- Bound to HB 30%
- Dissolved 10%

What does carbonic anhydrase do?
Carbonic anhydrase located within red blood cells
- CO2 + H2O - H2CO3 - H+ and HC)3-
- Carbonic anhydrase converts CO2 into HCO3- within the red blood cell close to the tissue
- This liberates H+ ions (increasing acidity) which bind to HB causing the further release of O2 (Bohr effect)
Chloride shift = the HCO3- ions are transported out of the cell in exchange for CL-
Note the reverse happens at alveoli.

What is the Haldane effect ?
Haldane effect
- CO2 binds to a different site then oxygen = CO2 binds to the globin site where as O2 binds to the heme component.
- removal of oxygen from HB in tissues increases affinity for CO2 - favouring the loading of CO2 in tissues

What is cyanosis ?
refers to a blue-purple discolouration of the skin and mucous membranes, caused by elevated concentration of deoxygenated hemoglobin.
Name the three components that regulate the respiratory system ?
Respiratory system
Regulated tightly to maintain concentration of O2, CO2 and H+ at constant levels independant of varying external conditions
- Control centre = rhythmic neural discharge for automatic control
- Chemical receptors = regulate the magnitude of ventilation to match physiological needs
- modification of respiration to meet other physiological needs

Describe the central respiratory centre

Pons and medulla central respiratory centre
- rhythmic neural discharge for automatic control
- respiratory rhythmicity originates in the brain stem : respiratory central pattern generator located pons and medulla
- neurons in medulla signals inspiratory muscles
- Stimulate diaphragm via phrenic nerve
- stimulate intercostal muscles by the intercostal nerve.

How does the central respiratory centre regulate expiration ?
Expiration
- at rest expiration is due to inhibition of inspiratory neurons
- when physiological demand increases expiratory neurons become activated to enhance ventaltion
- Signal nerves innervate the internal intercostal muscles and abdominal muscles

Describe how the higher brain regions can act on the respiratory centre to alter respiration ?
Voluntary control is innervated by the cerebral cortex
- phonation, swallowing, partuition and defacation have altered respiratory signals voluntary control
- cerebral cortex

Where are respiratory central and peripheral chemoreceptors located, and what affect do theses receptors have ?
Central chemoreceptors = medulla close to respiratory centre
Peripheral chemoreceptors = carotid bodies and aortic arch
Chemical chemoreceptors regulate the magnitude of ventilation to match physiological needs
- goverened by PO2, PCO2 and H+ in arterial blood which is detected by chemoreceptors.

Describe central chemoreceptors and how they are activated ?

Central chemoreceptors
- situated in the medulla close to the respiratory centre
- Hypercapnia (high CO2) is the primary driver for activation of central chemoreceptors its action is carried out through H+
- CO2 can not cross the blood brain barrier, where as H+ can
- Increased H+ in interstitual fluid of the brain stimulates central chemoreceptors
- stimulates hyperventilation

Describe peripheral chemoreceptors and how they are activated ?
Peripheral chemoreceptors
- Located the aortic arch and carotid bodies
- stimulated by a decrease in arterial PO2, increase in H+ (especially non CO2 generated as in metabolic acidosis) and increase in PCO2
- hyperventilation by stimulating the respiratory center in the medulla
- increases ventilation
Note - adjustment for acid base balance stimulated by an increase in H+. will stimulate peripheral chemoreceptors to a major extent and to a lesser extent central chemoreceptors. Diabetes mellitus

Describe the evolution of the cardiovascular system ?
Evolution of the cardiovascular system
- simple small organsisms simple diffusion
- multicellular flow through system eg sponges
- Fish simple two chambered heart
- Amphibians three chambered heart - lead to a seperate circuit for the first time - one ventricle two atrium - some mixing of deoxygenated blood and oxygenated blood in the one atrium
- mammals, birds and crocodiles eveolved a four chambered heart - two atria and two ventricles - oxygenated and deoxygenated blood completely seperated

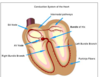
Name the four layers of the heart ?
Pericardium - contains fluid
Epicardium
Myocardium
endocardium

Describe the heart valves of the mammalian heart and their function - location ?
Heart valves
Functions to ensure one way flow of blood and prevent mixing of oxygenated and deoxygenated blood
Pulmonary valves =
Atriventricular valves = prevented from closing by chordae tendineae supported by papillary muscles. (tricupsid valve)
- the valves open and close passively
- forward pressure gradient opens valves
- backward pressure gradient closes valves
- valvular disease will reduce cardiac output

Describe the structure of the myocardium in the mammalian heart ?
Myocardium
- middle layer the thickest
- consits of myocardial cells which comprise 99% of the heart
Myocardial cells
- cardiac muscle cells
- excitable, striated, mononucleated and has abundant mitochondria
- intercalated disc = gap junctions which allow molecules and small ions to move between cells
- The intercalated disk allows quick spread of action potentials
The myocardium acts as functional syncytium contracts as a single unit.
Atrial and ventricular syncytia are seperated by a layer of connective tissue

Describe auto-rythmic cells location and their pathway through the heart ?
The heart depends on auto-rythmic (pacemaker cells) for rythmic beating, and does not require activation by the nervous system.
- situated in the sinoidal node, aventricular node and conduction pathways of the heart
- do not have a constant resting membrane potential
- pacemaker activity
- slowly depolarises between action potentials - declines to the firing level - pace maker potential or pre potential
The SA node is the usual pace maker as HR is determined by the fastest pacemaker.
Describe phase four action potential in the SA node ?
Phase four = pre potential

Funny Na+ channels open allowing Na+ into the cell - this is unusual as it occurs while the cell is relatively polarised (if)
This causes transient Ca2+ channels to open which causes further depolarisation (ica), which occurs during the second half of phase four.
Describe what happens during phase 0 and 3 during the action potential of the SA node ?
Phase 0 rapid depolarisation
- occurs due to opening of long lasting voltage gated CA2+ channels once the threshold potential is meet -40mV
Phase 3 repolarisation
- Due to opening of K+ channels and closing of Ca2+ channels
- as the membrane reaches -65mV, the if Na+ channel start to reopen.

Describe the parasympathetic activity on the SA node ?
Parasympathetic
- Acetylcholine
- Parasympathetic nerves cause a slower rate of rise in the pacemaker cells
- phase four SA node prolonged
- deacrease in HR

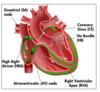
Describe the conduction pathways within the heart ?
Conduction pathway within the heart
- SA node - internodal path - AV node - AV bundle (HIS bundle) - bundle branches and purkinje fibres
- atrioventricular node delays the impulse (AV node delay)
- AV node and AV bundle provide the only route for the propagation of action potentials from the atria to ventricles
- AV bundle splits into left and right bundle branches
- purkinje fibres arising from the bundle spread impulse over the ventricular wall
- rapid to allow synchronous depolarisation.
Describe the five phases of the action potential in the cardiac contractile cell ?
Contractile cell
- Phase 0 rapid depolarisation
- opening of voltage gated Na+ channels
- Phase 1 initial rapid repolarisation
- opening of transient K+ channels
- Phase 2 plateau phase
- opening of long lasting Ca 2+ channels
- Phase 3 rapid repolarisation
- K+ influx by the opening of voltage gated K+ channels
- Phase 4 resting phase

In cardiac muscle what is the refractory period, compare this to the refractory period in skeletal muscle ?
Refractory period
Occurs immediately after the initiation of an action potential, and last until the action potential is complete
- no response to further excitation until the refractory period has ended.
Contrast skeletal and cardiac refractory period
- skelatal short 5 msec
- prolonged in cardiac muscle 300msec
- contractile time in cardiac muscle is longer than in skeletal muscle (as action potential duration is longer) this ensures adequate time for the ejection of blood

What are the benefits to having a prolonged refractory period in cardiac muscle ?
Refractory period
- cardiac muscle can not be restimulated until contraction is over - unable to have sustained contraction or summation of contraction
- can not fatigue cardiac muscle
- provides sufficient time to empty and refill cardiac chambers

What is an electrocardiogram ECG, and how do we attch it ?
ECG is the record of electrical activity of the heart
- word ‘lead’ in ECG recording refers to the tracing of the voltage difference between two electrodes
- ECG waveforms are produced by momentary changes in voltage differences during the spread of cardiac excitation.
Connection
- Lead 1 right foreleg to left foreleg
- Lead 2 right foreleg to left hindleg
- Lead three left foreleg to left foreleg

Describe normal ECG waves ?
Waves
P wave
- atrial depolaristation - small positive deflection
- atrial repolarization is a slow process, hence dose not usually produce a significant visible wave (may be obsecured by QRS)
QRS complex
- ventricular depolarisation
- Q first negative deflection, R large positive deflection and S negative deflection following R.
T wave
- ventricular repolarisation
- pattern of ventricular repolarisation varies between animals and may be positive or negative.

Describe the mechanical events which follow the electrical events on an ECG ?
Mechanical events which follow
- p wave followed by atrial contraction
- QRS followed by ventricular contraction
- T wave followed by ventricular relaxation
The delay of cardiac impulse conduction at the AV node prevents overlap of atrial and ventricular contraction

In an ECG describe the PR interval, if this interval was prolonged what disease would you expect ?
PR interval
- Longer than normal signifies a delay in impulse from SA node to ventricles
- Duration of conduction from the SA node to ventricles

QT interval in an ECG what does this signifiy ?
QT interval
- electrical activity in ventricles - repolarisation and depolarisation
- interval of QRS to T wave
- influenced by electrolyte balance, drugs, ischemia

Describe the RR interval what does it signify ?
RR interval
- interval between two successive RR
- duration is equal to one cardiac cycle
- HR/min = 60/RR interval

What is a Wiggers diagram, and describe the four phases of a Wiggers diagram ?
The four phases of a Wiggers diagram

1 = ventricular filling + gradual rise in left ventricular pressure
2a = isovolumetric contraction phase = steep rise in pressure as both valves remain closed
2b = ejection phase + left ventricular pressure is higher than in the aorta
3 = isovolumetric relaxation phase + no change in volume + both valves remain closed + steep drop in ventricular pressure
Describe a first degree AV block - conduction block
First degree block
- AV node block is a common dysfunction of cardiac impulse conduction
- may be caused by cardiac trauma, toxins, bacterial infections etc
- Three dgrees of severety of AV block are recognised
First degree AV block
slowed conduction through AV node
PR interval prolonged

Describe a second degree, and third degree AV block ?
Second degree AV block
- some P waves are not followed by a QRS complex
As the degree of AV block increases until the AV node fails completely and no QRS wave is seen
Third degree AV block
- complete conduction block
- no impulse goes through the AV node
- the atrium and ventricles beat at their own intrinsic rate
- purkinje fibres initiate ventricular contraction
- cardiac out put and blood pressure is compromised - animals will be weak and may collapse.
- treat by using a pace maker

Describe a cardiac arrhythmia and how they may be identified on an ECG ?
Cardiac arrhythmias
Any variation in the normal rythm of the heart , requires treatment if animal develops clinical signs such as syncope
- impaired impulse formation
- impaired impulse conduction
As seen on an ECG
- no P wave
- P wave not followed by a QRS
- abnormal P wave
- prolonged PR interval
- irregular waves as in ventricular fibrillation

Describe a cardiac arrhythmia - ectopic pacemakers and atrial fibrillation ?
Atrial fibrillation
- frequency of the generation of action potentials is too high
- common in older animals and horses
- continuous random passage of action potentials within the atrium
- well tolerated, few AP manage to get through the AV node
Complications = blood may pool in parts of the atria forming clots

Describe ectopic pacemakers - ventricular fibrillation ?
Ventricular fibrillation
- electric chaos, random voltage fluctuations generated by fibrillating ventricles
- no coordinated ventricular contraction
- reduced cardiac out put and arterial pressure
Defibrillation = CPR

Describe parasympathetic innervation of the heart invlude function, receptors and the location of where the nerves act ?
Parasympathetic innervation
- right vagus supplys SA node
- left vagus supplys AV node and Bundle of His
- Inervation of atrial muscles, but very few connections to ventricular muscle
Function
- reduce HR
- reduce conduction of impulses
- Increase delay in AV node
Vagus nerve acts by releasing acetylcholine which acts upon muscarinic M2 receptors on the heart muscle

Describe the sympathetic innervation of the heart, including function, what receptors it acts upon and where the nerves are located ?
Sympathetic innervation
- SA and AV node
- Bundle of HIS branches and ventricular muscle
Function
- quicker, stronger and faster
- increase HR
- increase force of contraction
- speeds up relaxation
- increases cardiac conduction velocity of impulses
Sympathetic nerevs act upon beta one and two in ventricular muscle, which respond to circulating adrenaline and noradrenaline

Define cardiac output and how is it determined ?
Cardiac out put
It is the volume of blood pumped out by each ventricle per minute
- both ventricles simulaneously pump the same amount of blood
- continually adjusted to meet biological needs
cardiac out put (vol/min) = stroke vol (vol pumped) * HR (beats/min)

Define cardiac reserve ?
Cardiac reserve
The maximum percentage that the cardiac output can increase above normal is known as the cardiac reserve
- cardiac out put can be increased up to a limit
- low cardiac reserve may indicate heart disease such as cardiac failure

Define ejection fraction ?
Ejection fraction
This can be defined as the end fraction of duystole that is ejected juring systole
SV/EDV = EF
- normal EF values between 50% and 80%
- index of ventricular function

What is stroke volume and what three factors dose it depend on ?
Stroke volume = is the volume of blood pumped by each ventricle per beat.
SV = EDV (end dystolic vol) * ESV (end systolic volume
Stroke volume depends upon three factors
- pre load
- after load
- cardiac muscle contractility

Describe preload and what factor affects it?
Pre load = extent of diastolic filling or end diastolic volume is preload.
- the strength of contraction is increased by increased filling of the heart
- increase in preload increases force of contraction
- within limits stretching of the ventricular fibres optimizes overlap between myosin and actin filaments increasing the strength of contraction.
- also increases the amount of CA2+ released from the sacroplasmic reticulum.

What is afterload, and how can it be adjusted ?
Afterload = is the tension developed in the ventricular wall during ejection
- determined by arterial resistance (arterial pressure)
- increase in afterload - the more difficult it becomes for ventricles to eject blood
- sustained high arterial pressure increases left ventricular workload - eventually leading to heart failure
Higher afterload reduses stroke volume in a heart that is failing.

State the four functions of the kidney ?
The four functions of the kidney ?
- removal of waste materials
- maintenance of the composition of body fluids
- production of hormones (vitamin D3, renin and erythropoietin)
- production of pheramones

What is a nephron, and what is its functional components ?
The nephron is the function component of the kidney.
It is composed of
- glomeralus
- proximal collecting tubule
- distal collecting tubule
- collecting duct
- medulla and cortex of the kidney
- macula denser
- Bowmans capsule

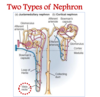
Name and describe the two different types of nephron ?

Two types of nephron
Juxtamedullary
- specialised for the formation of concentrated urine
- renal corpscles lie just above the junction of the cortex and medulla
- long hoop of Henle extends into the inner medulla
- supplied by vasa recta which runs parallel to the loop of Henle
- varies between species eg cat 100%, pig 3%
Cortical nephron
- renal corpuscles lie in the outer layer of the cortex
- short loop of Henle
- % of cortical nephrons varies between species
How is the renal system stimulated ?
Stimulation of the renal system
- supplied by sympathetic nerves
- primarily supply the afferent and efferent arterioles
- also proximal and distal tubules, loop of Henle and juxtaglomerula cells
- powerful stimulation decreses bllod flow
The effect is a increase in renin, increase in Na+ reabsorption and decrease in EBF/GRF

How is the vascularisation of the kidney unique, and what is the function of this unique system?

Vascularisation of the kidney and its function
- kidney highest blood flow per unit mass among major organs 20-25%
- mainly for the rate of glomerula filtration
- double capillary network in series
Glomerulus = high pressure capillary bed favors filtration (60mmhg)
Pertubular capillary network = low pressure capillary network (20mmhg) permits rapid reabsorption.
Note afferent arterioles are shorter and wider than efferent arterioles, which is required for the high pressure within the glomerulus.

Describe the three basic steps of urine formation ?
Glomerular filtration
tubular reabsorption
tubular secretion

How does the glomerular barrier prevent the filtration of proteins and cells?

All molecules and ions are filtered at the same concentration as in plasma except protein and cells.
What prevents protein and cells being filtered the glomerular barrier
- endothelium capillary (fenestrated negative charge)
- Basement membrane or basal laminar capillary (negatively charged, collagen and proteoglycans)
- epithelial cells of the Bowman’s capsule (negatively charged) which have podocytes

What is a podocyte ?
Podocyte
- Within the epithelial cells of the Bowman’s capsule
- has foot processes
- negatively charged
- prevents the filtration of proteins and cells

What determines the net filtration pressure ?

Net filtration pressure
- glomerula hydrostatic pressure
- Glomerula protein osmotic pressure (colloid osmotic pressure opposes filtration).
- hydrostatic pressure of the Bowman’s capsule (opposes filtration)
The colloid osmotic pressure of the Bowman’s capsule is negligible as proteins are not filterred in a healthy kidney.
The changes in glomerular hydrostatic pressure is the main means for physiological control regulation of GFR.

Describe the glomerular filtration ?

Glomerular filtration
- fenestrated capillaries
- high capillarie hydrostatic pressure
- capillary tuft inbetween two arterioles
The afferent arterioles are shorter and wider than efferent arterioles - which is required for high pressure within the glomerulas
- glomerular filtration is a passive process
- filtrate is identical to plasma (PH, osmolality) but protein free
*

Describe the juxta glomerular apparatus ?

Juxtar glomerular apparatus
- autoregulation
- GFR and RBF are primarily determined by the glomerular hydroastaic pressure
- constriction of afferent arteriole increases GFR, but severe constriction decreases GFR
Composed of -ve feedback mechanism
- juxta glomerular cells (granular cells). Located mostly around the afferent arteriole, and act to secrete renin
- Lacis cells which are located between the afferent and efferent arteriole. These cells are involved in the renin-angiotensin-aldosterone system.
- Macula densa - afferent arteriole or modified distal tubule. The macular densa detects changes in tubular fluid Na+ and Cl-

Desribe how GFR may be measured ?

Glomerular filtration rate
GFR is the sum of filtration rates of all nephrons = total glomerular filtration rate .
Measurement of GFR is the best single means of assessing kidney function.
Criteria for a substance to be used to measure GFR are
- freely filtered (not reabsorbed or secreted)
- non toxic, not metabolised or stored within the kidney
- substance which meet these criteria inulin, iohexol and endogenous creatine.
- Plasma creatine concentration is a good indicator of GFR as it is freely filtered, produced continuously and excreted in urine.

What is renal clearance ?

Renal clearance
It is a measure of the kidneys ability to remove substances from the plasma
- of a substance is the volume of plasma from which that substance is removed by the kidneys per minute.

Describe tubular function ?

Tubular function
Glomerular filtration is non selective (to a large extent) process but tubular reabsorption and secretion are highly selective processes.
- modulating the volume and composition of urine
- structure of each tubule section is adapted to its specific function
- transport proteins present on the cell membrane of tubular lining in each part of the tubule varies - which is the reason for the different function by different parts of the tubule.

Describe the process behind tubular reabsorption ?
Process of tubular reabsorption
Process
- driven by sodium - potassium ATPase (generates Na+ gradient inside of the cell)
- reasorption and secretion of most substances inside the tubule is driven by ATPase system.
- Cotransport - Na+ and solute same direction
- Counter transport - Na+ and solute moves in opposing directions
Process of solute transport
- paracellular reabsorption
- transcellular reabsorption
- carrier mediated transport

Describe carrier mediated transport across the apical membrane ?

Carrier mediated transport in the kidney
- 5-10% of mammalian genes code for transport proteins
- lack of causes many kidney diseases
- numerous transport proteins are crucial drug targets

Describe the glucose reabsorption and where it occurs ?

Glucose reabsorption in the proximal tubule
Normally glucose is completely reabsorbed by the proximal tubule
- secondary active transport, which prevents nutritive loss
- sodium ion and glucosetransported into PT cell by sodium-glucose transporter (SGLT) on luminal side
- glucose is then transported out of the cell by Glut2 transporter
- eventually glucose enters the blood

What is glycosuria, and what dose it cause ?

Glycosuria
It is the pressence of glucose in urine
- a common cause is diabettes mellitus due to rise in blood glucose conc
- may also occur in tubular two dysfunction (SGLT mutations)
- also causes an excessive water loss into the urine, a process called osmotic diuresis (osmotic effect of glucose)
- carrier mediated transport is saturable - renal threshold
filtered load > reasorbing capacity of the proximal tubule

Describe the function of the proximal tubule ?

Function proximal tubule
- 65% of filtered Na+, CL- and water reabsorbed
- osmotically reabsorbed
- reabsorbs glucose, amino acids, Na+, K+, CL-, Ca++ and HCO3-
- 40% of urea reabsorbed via pinocytosis
- secretes organic anions and cations.

Describe the function of the loop of Henle

Describe the function of the loop of Henle
Descending
- highly permeable to water and moderately to urea
Ascending part
- thin impermeable to water, but permeable to sodium
- thick reabsorbs 25% of Na+, Cl- and K+
Both thin and thick ascending parts are impermeable to water

Describe the function of the distal part of the tubule ?

Function of distal tubule

The first part of the distal tubule resembles that odf the ascending loop of henle - permeable to water and reabsorbing Na+ and Cl-
The late distal tubule and collecting duct reabsorb sodium and is impermeable to water.
Avid absorption of salts without water absorption produces a hypotonic tubule fluid, thus, these segments are sometimes called diluting segments.
Describe the function of the medullary collecting duct ?
Medullary collecting duct
Crucial in determining the final output of urine and solutes
- permeability to water depends on ADH
- permeable to urea contains urea transporters
- secretes hydrogen ions against a lrage concentration gradient

Describe the function of principle cells, intercalated disks and where are they located ?
Both principle cells and intercalated disks are located in the late distal tubule and collecting tubule
Principal cells
- reabsorb sodium from the lumen
- secretes potassium
- may become permeable to water in the pressence of ADH
Intercalated disks
- key role acid base balance
- alpha cells secrete H+, reabsorb bicarbonate
- Beta cells secree bicarbonate and reabsorb H+

The kidney acts to regulate four physiological parameters simultaneously, what are these parameters ?

Four physiological parameters
- water balance
- osmolality
- ECF volume
- blood pressure

Discuss Na+ reabsorption within the proximal tubule ?

Proximal tubule
- 65% of the mass of filtered sodium is reabsorbed
- isosmotic tubular fluid
Angiotensin 2
- enhances Na+ reabsorption from the proximal tubule
- early Na+ reabsoprtion is linked to nutrient transport and H+ secretion

Describe Na+ reabsorption by The thick ascending limb of loop of Henle and early distal tubule ?

Ascending limb and distal tubule.
Thick ascending limb reabsorbs Na+ and Cl- but is virtually impermeable to water.
- hypo-osmotic (more dilute fluid) tubular fluid when compared to the plasma
ADH vasopressin = enhances Na+ reabsorption from thick ascending limb

Describe the reabsorption of Na+ by the late distal tubule and collecting tube ?

Na+ reabsorption in the late distile tubule and collecting duct

Principal cells = Na+ entry from the lumen is via an ion channel epithelial sodium channel (ENaC)
Aldosterone = increases the absorption of Na+ and increases K+ secretion in principal cells
Describe the RAAS Renin-angiotensin, aldosterone system and what it achieves ?

Renin-angiotensin aldosterone system
- important salt conserving system
- important role in regulating Na+ balance
- ECF palsma volume
- regulation of arterial pressure.
Angiotensin two stimulates the production of
- ADH vasopressin, acts upon the ascending loop of Henle to incrase Na+ absorption
- aldosterone acts upon principal cells to increase Na+ absorption.

Identify the six effects of Angiotensin 2.
Angiotensin two acts to increase ECF volume in several ways. (defends against a decrease in ECF volume).
- increase water retension
- increase thirst
- vasocontriction of the systemic circulation
- stimulate secretion of ADH posterior pituitary
- stimulate secretion of aldosterone secretion
- increase proximal tubule Na+ absorption + increase action of principle cells to increase Na+ absorption
Aldosterone and ADH is released from the zona glomerulosa

Describe the actions of ADH (antidiuretic hormone) on the renal tubule ?
ADH
Acts to decrease volume and increase concentration
- increase in plasma osmolality (concentrated) results in increased secretion of ADH
- inserts urea transporters increasing urea uptake
- stimulates reabsorption of Na+ thick ascending loop of Henle
- Inserts aqau porins in the luminal membrane of principal cells increasing water reuptake
- negative feed-back mechanism

What is the affect of aldosterone on the kidney?
Aldosterone
