Paediatric Oncology Flashcards
what is cancer and its features?
- Abnormal cells dividing in an uncontrolled way
- Gene changes
- Stimulates own blood supply
- Local invasion
- Metastatic spread via blood or lymphatic systems
how common are cancers in childhood?
- Rare -1821 cases < 15 in UK (per year 2013-15)
- Scotland 130 / yr
- 1/500 pre age 14
- GP sees 1 in career
- 10-15 per DGH catchment/year
- <1% all cancers
- Boys slightly more than girls
In the current era over 85% of childhood cancers are cured
are are paediatric cancers classified?
- International Classification of Childhood Cancer (ICCC)
- Based on tumour morphology and (primary site)
- Standard classification is essential for comparing incidence and survival across regions and over time periods
Classify childhood cancer based on the cell of origin, which is different to adult tumours where they focus on the primary site
why do children get caners?
Most childhood tumours are sporadic so bad luck. In about 10% there may be a cause. This can be due to a genetic syndrome the environment or a previous treatment:
- Genes - Down, Fanconi, BWS, Li-Fraumeni Familial Cancer Syndrome, Neurofibromatosis
- Environment - Radiation, Infection
- Iatrogenic - Chemotherapy, Radiotherapy
Summary:
- Childhood cancer is rare but does happen
- Usually sporadic
- Need to think of it
what is the diagnostic journey of a child with cancer?

Who to be worried about?
- Immediate referral - unexplained petechiae, hepatosplenomegaly
- Urgent referral:
- repeat attendance, same problem, no clear diagnosis
- new neuro symptoms, abdo mass
•Refer (to doctor or for urgent investigation):
- rest pain, back pain and unexplained lump
- lymphadenopathy ………
what are the symptoms of a brain tumour in different children ages?

whata re some oncological emergencies?
- Sepsis / febrile neutropenia
- Raised ICP
- Spinal cord compression
- Mediastinal mass
- Tumour lysis syndrome
Sepsis/febrile neutropenia:
Infection is major cause of morbidity/mortality
what are the risks and what organisms may be responsible?
•Risks:
- ANC < 0.5 x 109
- Indwelling catheter
- Mucosal inflammation
- High dose chemo/SCT
- Pseudomonas aeruginosa
- Enterobacteriaciae eg E coli, Klebsiella
- Streptococcus pneumoniae
- Enterococci
- Staphylococcus
- Fungi eg. Candida, Aspergillus
how does sepsis present?
- Fever (or low temp)
- Rigors
- Drowsiness
- Shock - Tachycardia, tachypnoea, hypotension, prolonged capillary refill time, reduced UO, metabolic acidosis
how do you manage sepsis?
IV access
Blood culture, FBC, coag, UE, LFTs, CRP, lactate
CXR
Other - Urine microscopy / culture, Throat swab, Sputum culture / BAL, LP, Viral PCRs, CT / USS
ABC - Oxygen and Fluids
Broad spectrum antibiotics
Inotropes
PICU
what are the early and late signs of ICP?
HC = head circumfrance

how would you investigate increased ICP?
- Imaging is mandatory (if safe)
- CT is good for screening
- MRI is best for more accurate diagnosis
Children often need anaesthetic to get good quality imaging and don’t want to do this if worried if unsafe due to risk of death or coning
how should raised ICP be managed?
- Dexamethasone if due to tumour - Reduce oedema and increase CSF flow, 250 micro/kg IV STAT then 125 microg/kg BD
- Neurosurgery - urgent CSF diversion:
- Ventriculostomy – hole in membrane at base of 3rd ventricle with endoscope
- EVD (temporary)
- VP shunt
how would someone present with spinal cord compression?
- Symptoms vary with level:
- weakness (90 %)
- pain (55-95 %)
- sensory (10-55%)
- sphincter disturbance (10-35%)

SVC syndrome or SMS - how should it be investigated?
- CXR / CT chest (if able to tolerate)
- Echo
Left is mediastinal

what is the management of SVC syndrome or SMS?

what are the clinical features of tumour lysis syndrome?
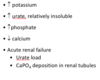
how do you treat tumour lysis syndrome?

What are the risks of treatment? (chemotherapy and radiotherapy - acute and chronic)

what may the later effects of a cancer be?

