Other inflammatory skin disease Flashcards
What’s exanthem?
Exanthem is a widespread rash occurring on the outside of the body and usually occurring in children
Cause: toxins, drugs, or microorganisms, an autoimmune disease
Examples: varicella-zoster, Scarlet fever, measles, rubella etc..
What’s toxic epidermal necrolysis?
Toxic epidermal necrolysis (TEN)
- a potentially life-threatening skin disorder
- most commonly seen secondary to a drug reaction
- the skin develops a scalded appearance over an extensive area
- TEN is severe end of a spectrum of skin disorders which includes erythema multiforme and Stevens-Johnson syndrome
Features of Toxic Epidermal Necrolysis
- systemically unwell e.g. pyrexia, tachycardic
- positive Nikolsky’s sign: the epidermis separates with mild lateral pressure

Drugs known to induce TEN
Drugs known to induce TEN
- phenytoin
- sulphonamides
- allopurinol
- penicillins
- carbamazepine
- NSAIDs
Management of TEN
- stop precipitating factor
- supportive care, often in ICU
- intravenous immunoglobulin used first-line
- immunosuppressive agents (ciclosporin and cyclophosphamide)
- plasmapheresis
- analgesia
*opthalmological input may be needed - if eye involved
* burns unit may be required for specialised skin care
Spot diagnosis

Urticaria

Characteristics of urticaria
Urticaria is characterised by:
- weals (hives)
- angioedema
Weal (or wheal)→ a superficial skin-coloured or pale skin swelling, usually surrounded by erythema (redness). Usually very itchy, it may have a burning sensation.
Pathophysiology of urticaria
- release of chemical mediators from tissue mast cells and circulating basophils
- these chemical mediators include histamine, platelet-activating factor and cytokines
- the mediators activate sensory nerves and cause dilation of blood vessels and leakage of fluid into surrounding tissues
- Bradykinin release causes angioedema
Causes of urticaria
- Acute viral infection — an upper respiratory infection, viral hepatitis, infectious mononucleosis
- Acute bacterial infection — a dental abscess, sinusitis, mycoplasma
- Food allergy (IgE mediated) — usually milk, egg, peanut, shellfish
- Drug-induced urticaria (IgE mediated) — often an antibiotic
- Drug-induced urticaria due to pseudoallergy — aspirin, nonselective nonsteroidal anti-inflammatory drugs, opiates, radiocontrast media; these cause urticaria without immune activation
- Vaccination
- Bee or wasp stings
- Widespread reaction following localised contact urticaria — rubber latex
*Severe allergic urticaria may lead to anaphylactic shock (bronchospasm, collapse)
*A single episode or recurrent episodes of angioedema without urticaria can be due to an angiotensin-converting enzyme (ACE) inhibitor drug
Diagnosis of acute urticaria
Acute urticaria
- short history of weals that last less than 24 hours, with or without angioedema
- A thorough physical examination should be undertaken to look for underlying causes
- skin prick tests and radioallergosorbent tests (RAST) or CAP fluoroimmunoassay may be requested if a drug or food allergy is suspected in acute urticaria
Weals vs fungal infection
WEALS: Oedamatous DERMAL in urticaria
Fungal: EPIDERMAL, scaly
Urticaria vs urticarial vasculitis
- Urticaria: comes and goes quickly (lasts for 24-48 hours)
- Urticarial vasculitis (looks like urticaria) but lasts for longer, has a bit of bruise; may affect any organ (as vasculitis) and requires biopsy

Classification of urticaria (timeframe)
- Acute → less than 6 weeks
- Chronic → more than 6 weeks (not associated with allergy)
Is urticaria associated with an allergy?
URTICARIA does not = allergy!
Urticaria may be a feature of anaphylaxis but not always
Management of urticaria
Non-sedating anti-histamine → x4 the usual dose cetirizine/loratadine
Describe the rash + diagnosis

Maculopapular rash (some flat some bumpy spots)
It’s characteristic of exanthem
*in children usually viral
*in adult e.g. drug reaction/ HIV seroconversion

Drugs known to (commonly) cause skin changes
- sulphonamides
- anticonvulsants
- penicillins
- allopurinol
- NSAIDs
*it may be 1-2 weeks delay in between starting the drug and rash; even if the drug has been stopped
Describe + diagnose

Haemorrhagic crusting of the lips
Typical for Steven-Johnson syndrome
Features of Stevens-Johnson syndrome
- prodrome of fever and respiratory symptoms
- two or more mucosal sites
- possible severe eye and oral involvement
- non-specific or targetoid eruption
- prolonged course

What’s that?
Causes, describe
Purpura (vasculitis eruption)

Causes: vasculitis, low platelets, meningitis, HSP etc.
Description: Shower of individual little spots, coalescence, non-bleaching
Name these lesions (each picture)
What disease are these associated with?


Name these lesions (each picture)
What disease are these associated with?


Name these lesions (each picture)
What disease are these associated with?


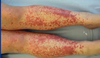
Spot diagnosis

Erythema Nodosum
- tender lumps
- inflammation of the fat
Causes of Erythema Nodosum
NO - idiopathic
D - drugs: sulphonamides, amoxicillin
O - OCP
S - sarcoidosis
U - UC, Crohn’s, Behcet’s
M - microbiology - strep, TB, viral
Causes of pyoderma gangrenosum
- nose, legs but also other sides
- Hx: pustule, a nodule that rapidly expands and ulcerates
- often multifocal (separate bits that may join up)
- very painful
Treatment: underlying cause, oral steroids

Overview of dermatomyositis
- an inflammatory disorder
- symmetrical, proximal muscle weakness and characteristic skin lesions
- may be idiopathic or associated with connective tissue disorders or underlying malignancy
- screening for an underlying malignancy is usually performed following a diagnosis of dermatomyositis
- polymyositis is a variant of the disease where skin manifestations are not prominent

Skin features of dermatomyositis
Skin features
- photosensitive
- macular rash over back and shoulder
- heliotrope rash in the periorbital region
- Gottron’s papules - roughened red papules over extensor surfaces of fingers
- ‘mechanic’s hands’: extremely dry and scaly hands with linear ‘cracks’ on the palmar and lateral aspects of the fingers
- nail fold capillary dilatation

Spot diagnosis

Heliotrope rash → feature of dermatomyositis
Spot diagnosis

Gottron’s papules → feature of dermatomyositis
Spot diagnosis

Erythema multiforme
- target lesions (for true target lesions at least 3 colours in a single lesion)
- viruses: herpes simplex virus (the most common cause), Orf*
- idiopathic
- bacteria: Mycoplasma, Streptococcus
- drugs: penicillin, sulphonamides, carbamazepine, allopurinol, NSAIDs, oral contraceptive pill, nevirapine
- connective tissue disease e.g. Systemic lupus erythematosus
- sarcoidosis
- malignancy

Spot diagnosis

Inverse Flexural Psoriasis
- scale is lost in moist flexural sites
- fissure in the crease
- usually in the natal cleft
Treatment: similar to psoriasis; mild- moderate topical steroids
(no vit D or tar as it will irritate delicate areas)
Spot diagnosis

Tinea corporis
Treatment for this

Do nothing - Seborrhagic keratoses
If not sure what’s that - refer to dermatology
- well-demarcated
- depressions on the surfaces
- inclusion cysts (depigmentation)
Treat only if symptomatic: curettage, freeze
Diagnosis?
(unwell patient)

Necrotising fascitis
Diagnosis?

Superficial BCC
- looks like a red scaly plaque with no characteristic features
- biopsy it - to be sure
*this characteristic one - pearled age
* do not use cryotherapy for it
* imiquimod, incision, curettage used
Diagnosis?

It could be BCC or SCC
*rather SCC though due to keratin bits
Treatment to it?
Clue: Pt can’t go to work

Eczema infected with impetigo (in this case impregnated contact dermatitis)
- scaling
- diffuse over palmar surfaces
- golden crust
Treatment: oral antibiotics to cover strep and staph, potent topical steroid
Ix: swab, do a patch test (type IV delayed-type allergy)
lady is well, no other symptoms

Rosacea
- papules within redness
Treatment: oral tetracyclines, topical metronidazole
*but problem will be recurrent
