Neuro - MS Flashcards
Demographic of MS:
Age of onset?
Gender?
Demographic of MS:
15-45 years old
70% female
What is the most common form of ms?
50% of these patients convert to ____ ____ MS within 10 years, if ___ modifying therapy is given.
Relapsing-remitting MS (RRMS) is the most common form at initial diagnosis: 85%
50% of RRMS patients convert to secondary progressive MS (SPMS) within 10 years, if NO modifying therapy is given.
Natural history of MS:
- What does the green line indicate?
- What does the purple line indicate?
- Red line and yellow aarows?
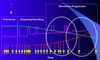
Natural hisotry of MS
- The green line measures brain volume
- The purple line shows relapses and impairment
- The red line and yellow aarows indicate activity of MRI
EDDS:
- What does this stand for?
- Level 0 = ?
- Level 5 = ?
- Level 10 = ?
EDDS:
- Expanded disability status scale
- Level 0 = normal
- Level 5 = reduced ambulation
- Level 10 = death
What type of MS does the graph represent?

The graph represents relapsing-remitting MS (RRMS)
What type of MS does the graph represent?

This is secondary progressive MS
What type of MS does the graph represent?

This is primary progressive MS
What type of MS does the graph represent?

This is progressive relapsing MS
Relapsing-Remitting MS (RRMS)
- What is it defined by?
- How does remission occur?
Relapsing-Remitting MS (RRMS)
- It is defined by “attacks” (flare ups/exacerbations/relapses) that last greater than or equal to 24 hours. Symptoms may take up to a month to resolve
- Remission occurs either spontaneously or with treatment
Progressive MS
- What is primary progressive MS (PPMS)?
- What is secondary progressive MS (SPMS)?
- What is progressive relapsing MS (PRMS)?
Progressive MS
- PPMS: (10%) Progressive deterioration without remission
- SPMS: develpos in approx. 50% of untreated people with RRMS; slow progressive neurological deterioration with or without occasional acute flare-ups/remissions/plateaus
- PRMS: (5%) progressive from the start (with acute flare-ups) and continued deterioration between relapses
Benign/Mild MS
- Considered a subset of what MS?
- Definition?
- 10 year follow up?
Benign/Mild MS
- Considered a subset of RRMS
- No accepted definition (no restriction of activity at >10 years, able to work after 20 years.. etc etc)
- Only 10-20% maintain a true mild course. Benign MS does not always remain benign.
Benign MS
Favorable:
- Age of onset?
- Area of involvement?
- Area/nature of first attack?
- Remission duration? Gender?
Benign MS
Favorable
- Before the age of 40
- Isolated involvement
- Optic neuritis, sensory, brainstem
- First remission duration > 1 year; female
Benign MS
Unfavorable:
- Age?
- Areas of involvement?
- Area/nature of first attack?
- Gender?
Benign MS
Unfavorable:
- Older than 40
- Multiple areas of involvement
- Motor, cerebellar, sphincter
- Male
Pathology of MS:
- Immune mediated in ____ susceptible individuals
- ______ leads to slower nerve conduction
- Where do lesions occur?
Pathology of MS:
- Immune mediated in genetically susceptible individuals
- Demyelination leads to slower nerve conduction
- Lesions occur in optic nerves, cerebellum, cerebral cortex, periventricular white matter, spinal cord, and the brain stem.
Cause of Demyelination and Axonal Loss:
Activation of autoreactive ____ ___ cells in the peripheral immune system. There is then migration of autoreactive ___ cells into the ____. This is followed by in situ reactivation by myelin autoantigens and activation of _____ and ___ cells. There is secretion of _____ ____. The terminal result is inflammation, _____, ____ transection, and ____.
Cause of Demyelination and Axonal Loss:
Activation of autoreactive CD4+ T cells in the peripheral immune system. There is then migration of autoreactive TH1 cells into the CNS. This is followed by in situe reactivation by myelin autoantigens and activation of macrophages and B cells. There is secretion of proinflammatory cytokines. The terminal result is inflammation, demyelination, axonal transection, and degeneration.
What are the red arrows pointing at?

The red arrows indicate MS plaques
Lesions of MS
- What are active lesions characterized by?
- What are chronic active lesions characterized by?
Lesions of MS
- Active lesions are characterized by abundant and evenly distributed MHC II cells and myelin-protein positive inclusions within macrophages
- Chronic active lesions are characterized by MHC II that are abundant at the edges of lesions and less frequent in the center
Diagnosis:
Ultimately what type of diagnosis?
Diagnosis:
Ultimately a clinical diagnosis - there is no definitive lab test
Most common presenting symtpoms?
a. Sensory symptoms in arms/legs - 33%
b. Unilateral vision loss - 16%
c. Multiple symptoms at onset - 14%
Diagnoses that mimic MS:
- Infections?
- Inflammatory?
- Metabolic?
- CNS ____
- 3 others?
Diagnoses that mimic MS:
- Lyme disease, neurosyphilis, HIV, HTLV-1
- SLE, Sjorgren’s, Sarcoidosis
- Vitamin B12 and E deficiencies
- CNS Lymphoma
- Cervical spondylosis, motor neuron disease, Myasthenia gravis
CSF in MS:
- How many cells per ml? Type of cell?
- If the cell count is greater than 50/ul consider other ____
- CSF protein? IgG? Oligoclonal bands?
- What is possible to note with Oligoclonal bands?
CSF in MS:
- 5-15 cells/ul; mostly T- lymphocytes
- etiology
- Protein = normal; IgG = elevated; OCB = often detected
- Number of bands may increase with disease duration
Symptoms:
- Inflammation of the optic nerve can cause?
- Brain stem lesions may cause changes in?
- Cerebellar lesions may cause?
- Spinal cord lesions may cause?
Symptoms:
- Inflammation of the optic nerve can cause retrobulbar pain, color desaturation, and visual loss.
- Brain stem lesions may cause changes in eye movement, vertigo, dysarthria, dysphagia, and facial weakness.
- Cerebellar lesions may cause ataxia and tremor.
- Spinal cord lesions may cause bowel, bladder, and sexual dysfunction, and spastic gait difficulties
Symptoms:
- Cerebral and corpus callosum lesions, as well as generalized brain atrophy, may cause?
- Common symptoms in diagnosed MS can include?
Symptoms:
- Cerebral and corpus callosum lesions, as well as generalized brain atrophy, may cause cognitive dysfunction.
- Fatigue, Pain, Spasticity, Elimination dysfunctions, Cognitive impairment, and Sexual dysfunction
McDonald diagnostic criteria:
- What is traditional diagnostic criteria?
- Outcome of the diagnostic workup should yield 3 of the following?
McDonald diagnostic criteria:
- Preserve traditional diagnostic criteria of 2 attacks of disease separated in space and time.
- 1 Gd-enhancing lesion or 9 hyperintense lesions, 1 or more infratentorial lesions, 1 or more juxtacortical lesions, or 3+ periventricular lesions
