Name that scan! Flashcards

I-131 scan more metastatic thyroid cancer, beta minus decay
uptake in the thyroid shows star artifact along with multiple metastatic sites

F18- NaF

Tc-99m MDP scan,
MOA: adsorption to crystals in bone matrix

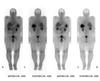
In-111 tagged WBC scan
hot spleen!!
two varieties of WBC scans: Tc-99m and In-111
Tc-99m WBC scan is preferred in kids because shorter half life (lower dose in kids) AND higher quality imaging (better spatial resolution for smaller parts)
In-111 has a longer half life –> more delayed imaging
In-111 –> less bowel uptake so preferred to evaluate for IBD


In-111 WBC in Crohns diseae with abscess


I-123 whole body pre-treatment
medium energy detector (not as crappy picture as I-131)

post thyroid ablation
what uptakes differs between pre and post treatment iodine scans?

post treatment: liver uptake (physiologic) is present in post treatment scan which is never present pre-treatment
can also see breast and colon uptake as in this case



normal distribution of Ga67


I-123 MIBG

I-123 MIBG scan. Normal or abnormal?

super abnormal. you shouldn’t see the bones at ALL. if you see bones on MIBG scan –> bone mets


tc99m O4 (pertechnetate)



Tc-99m MDP

Tc-99m sulfur colloid

Tc-99m sulfur colloid scan, posterior image (spleen on screen left)
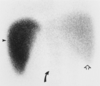
colloid shift = portal HTN
typically on SC scan the liver = spleen –> portal HTN the blood is shunted to the spleen –>
spleen > liver


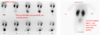
tagged RBC scan to look for bleed
Flow images of red blood cell labeled 99m-Tc gastrointestinal bleed scan: Chronological first site of bleed localized to distal ileum (arrow head) and proximal jejunum as primary site of bleed (arrow)
https://www.wjnm.org/viewimage.asp?img=WorldJNuclMed_2013_12_3_111_136735_f1.jpg

free tech in a meckel scan


altered biodistribution of MDP due to radiochemical impurity (free tech)

f-18 fdg pet

tc99m sestamibi

whole body sestamibi


F-18 fluciclovine PET (axumin)
taken up via the human l-type amino acid transporter and alanine-serine-cysteine transporter systems
uptake
in tissues that produce proteins or process amino
acids. l-type amino acid transporter and alanineserine-cysteine transporter systems
The most intense physiologic tracer uptake is seen in the pancreas (Fig 2). However, this uptake decreases within 15 minutes after injection of the radiopharmaceutical –> becomes more intense in the liver
moderate salivary gland and pituitary gland uptake and variable mild to moderate bowel activity
Liver is the critical organ


F-18 fluciclovine PET (axumin)
you have to image fluciclovine very soon after injection and scan from the pelvis up - start the scan before concentration in the urinary system

xe133 ventilation
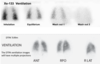

dtpa Tc99m ventilation scan


in111 DTPA
CSF scan. Radiotracer injected intrathecally
looking for delayed clearance (NPH) or shunt malfunction
How big are the particles?

Tc99m-MAA (microaggregated albumin)
10-100 micrometers
Tc-99m MAA

Shunting through AVMs –> systemic circulation
should only see MAA uptake in the lungs, if see it systemically it means there is a R –> L shunt
What does the red arrow point to?

hepatic steatosis
Xe-133 uptake in the liver

Gastric emptying study
Tc99m Sulfur colloid
standarized meal of eggs (radiotracer mixed in eggs) and toast


Tc99m-MAG3
you can see the various phases as it enters, transits, and excretion
Look for time activity curve




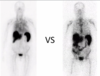

In-111 octreotide

In-111 octreotide

MIBG



MIBG

In-111 octreotide
case of metastatic carcinoid. Liver mets. carcinoid tumor in RLQ at TI

In-111 WBC scan
if this were a Tc-99m scan would see bladder, kidneys, and gut

Tc-99m DMSA

Tc-99m HMPAO WBC scan
if see gut uptake < 24 hrs (in the 4hr range), it is suggestive of IBD or colitis/enteritis


sestamibi

variable appearance of Ga-67
lacrimal gland and bowel uptake is variable

sestamibi with delays
bowel uptake decreases over time with sestamibi, so if using for the heart you have to delay so hepatobiliary uptake doesn’t get in the way

Tc-99m hmpao WBC scan
gut and bladder activity mean Tc-99m HMPAO

In-111 octreotide

Ga67
shitty bone scan plus liver

In-111 WBC
no gut or bladder uptake

octreotide

In-111 octreotide
absent spleen