Mitral Valve Disease Flashcards
mitral valve
- discuss its anatomical structure and location in the heart.
- under physiological conditions - when is it open and how wide does it open?
-
structure: a bicuspid valve made of 2 leafelets
- its opening is enclosed by a fibrous ring
- its leafelets are anchored by chordae tendinae to papillary muscles on the left ventricular wall
- location: in beween the LA and LV
-
open: during diastole
- this allows for filling of the left ventricle
- normally opens to a cross sectional area of 4-6 cm2
- cross sectional area of mitral valve
- what is normal?
- when do we start to see blood flow impairment?
- when does the valvular area become “critical”?
- how do we determine this area?
- normal cross sectional area: 4-6 cm2
- blood flow impairment seen at < 2 cm2
- symptoms start to present at this area
- valve area becomes critical < 1 cm2
cross sectional area determined with echocardiogram.
what is mitral stenosis?
decreased pliability of the mitral valve leafelets that impedes blood flow from the LA to LV
what are the major causes of mitral stenosis?
- rheumatic fever - #1 cause
- congenital
- aging with annular severe calcification
- SLE (lupus)
- RA (rheumatoid arthritis)
discuss the etiology of rheumatic fever
- what sex/demographics does it effect most
- what valvular diseases can it lead to
- # 1 cause of mitral stenosis worldwide
- 40% of valvuar manifestations of RF are mitral stenosis, and the remainder are mitral regurgitation or aortic valve disease.
- theses valvular manifestations usually present a few years - 20 years after initial infection
- 40% of valvuar manifestations of RF are mitral stenosis, and the remainder are mitral regurgitation or aortic valve disease.
- demographics: most prevalent developing countries
- sex: seen more in females > males
- discuss the major gross morphological changes seen in rheumatic valvular disease?
- what changes are characteristic of early vs end stage rheumatic valve disease?
i believe these are referring to changes in the mitral valve*
- major changes:
- thickening of valve leaflets
- fusion of comissures
- chorda tendinae shortening/thickening
- stage-specific features:
-
early
- leafelets flap open in a “curved over” manner due to restriction of motion at their tips.
- this causes an opening snap on ascultation
- leafelets flap open in a “curved over” manner due to restriction of motion at their tips.
-
as diease progresses:
- symmetric fusion of comissures results in a small, central oval orifice during diastole
-
end stage:
- leafelets can be so fibrotic/stiff they cannot open/shut
-
early
pathogenesis of rheumatic valve disease
it is an abrnomal immune response to group A streptococcal pharyngitis
what criteria must be met to diagnose rheumatic valve disease
- must see 2 major criteria OR 1 major + 2 minor criteria
- major criteria
- carditis
- polyarthritis
- erythema migratorum
- subcutaneous nodules
- chorea (uncontrolled movement)
- minor criteria
- fever
- arthralgia
- previous rheumatic fever/known rheumatic heart disease
- major criteria
what clinical presentations might indicate carditis?
- pleuritic chest pain
- friction rub
- heart failure
carditis is one of the major criteria for dx of rheumatic valve disease
what valves are most/least likely to be effected by rhuematic valve disease
- most likely = mitral/aortic valve
- least likely = pulmonic valve
what physiological changes are seen in mitral stenosis
- mitral stenosis = impaired flow from LA to LV during diastole. blood backs up in LA, doesn’t make it to LV. this leads to:
- LA pressure increase
- LA enlargement
- LV filling dimished
- this decreases end diastolic volume (preload) –> decreases stroke volume –> thus decreases cardiac output
- (CO = HR x SV)
- this decreases end diastolic volume (preload) –> decreases stroke volume –> thus decreases cardiac output

clinical presentation of mitral stenosis
- mild vs moderate
- mild stenosis = typically asymptomatic
- moderate stenosis (valve area 1-2 cm2) = exertional dyspnea and fatigue
- other clinical manifestations:
- chest pain
- atrial fibrillation/palpatitations
- stroke (18 x higher risk in these pts)
- right sided heart failure
- presents w/ edema, ascities, liver failure
- hoarseness (ortner’s dynrome)
- dysphagia
- hemoptysis from ruptured bronchial veins
what two cinical manifestations of mitral stenosis are due to LA enlargement?
- orntner’s syndrome: hoarseness due to the LA enlarging and putting pressure on the recurrent laryngeal nerve
- dysphagia: trouble swallowing due to LA enlarging and impinging on the esophagus
what kind of heart failure is seen in mitral stenosis & why?
what other clinical manifestations typically present alongside this heart failure?
- right sided heart failure
- blood back up into LA backs up into lung and then creates a huge afterload that the right heart must overcome.
- right sided HF can present with:
- edema*
- JDV*
- ascites
- liver failure
discuss key exam findings indicative of mitral stenosis
- what sounds will heard on ascultation?
- other findings
- ascultation
-
murmurs/sounds:
- loud S1 (mitral valve closure)
- opening snap (mitral valve opening) after S2 (aortic valve closure)
-
low-pitched diastolic flow murmur
- caused by turbulent blood flow thru valve
- i_rregular heart rhythm_
-
murmurs/sounds:
- other findings:
- signs of right sided heart failure
- periperal edema
- JVD
- stroke symptoms:
- facial drooping
- weakness on one side of the body
- signs of right sided heart failure
define the clinical significance of the “opening snap” heard on ascultation of a pt with mitral stenosis
- opening snap
- often heard in the early phase of rheumatic valve diease
- this sound is caused by the restriced motion of the diseased valve leafelets during mitral valve opening, which occurs after S2 (aortic valve closure)
- the shorter the interval between S2 and the “opening snap” the more severe the mitral stenosis
label these components of a stethoscope. what is purpose/proper orientation of each component


- when ausculating a patient with possible mitral stenosis
- what part of the stethoscope should you listen with and where on the heart should you place it?
- how should the patient be positioned?
- listen to apex of heart with the bell of the stethoscope
- place patient in left lateral decubitus
what is the “standard” diagnostic test for mitral stenosis
echocardiogram
echocardiogram for dx of mitral stenosis
- what types of echocardiograms can be done and in what circumstances?
- what can an echocardiogram tell you?
- echocardiogram = standard diagnostic test for mitral stenosis
- two possible views:
- transthoracic - usually preferred
- transesophageal (TEE) - preferred when 1. it is difficult to view valves or 2. we’re assessing for vegetations/thrombus
- echocardiogram is key to tell you:
-
degree of stenosis
- mild: mitral valve area > 1.75 cm2
- moderate: mitral valve 1.25 -1.75 cm2
- severe: mitral valve < 1.0 cm2
- pressures across valves/heart chambers
-
degree of stenosis
- two possible views:
other than an echocardiogram - what other diagnostics tests can be done to assess mitral stenosis and under what circumstances?
- EKG - useful if there is an irregular rhythm. could show
- LA enlargement
- right axis deviation
- RBBB
- cardiac catheterization - used if echocardiogram is undiagnostic. can tell you pressure in LA/LV
- exercise test stress - to induce exertional symptoms
when to do a cardiac catheterization in diagnosis of mitral stenosis/what can it tell you?
- do if echocardiogram is diagnostic
- can tell you pressure of LA/LV
when do an EKG if the diagnosis of mitral stenosis/what it can tell you
- do if there is an i_rregular rhythm_
- can show:
- LA enlargement
- right axis deviation
- RBBB
how to treat asymptomatic mitral stenosis
- generally, no treatment.
- unless:
- there is severe pulmonary artery HTN OR new onset atrial fibrillation, in which case:
- control HR with beta blocker/CCB
- and give warfarin (anti-coagulant) if their INR is 2-3
- they need a percutaneous balloon mitral valveotomy
- there is severe pulmonary artery HTN OR new onset atrial fibrillation, in which case:
how to treat heart failure secondary to mitral stenosis
give diuretics
how to treat mitral stenosis in patients with exertional symptoms
(what methods are preferred vs not preferred)
- NOT preferred: percutaneous balloon mitral valcotomy
- preferred:
- open/closed surgical mitral valvotomy
-
open heart mitral valve replacement
- mechanical mitral valve:
- these patients are given lifelong warfarin (comoudin) anticoagulant
- bioprosthetic mitral valve:
- for patients older than 65 or who can’t take anti-coagulants
- mechanical mitral valve:
- when are valve replacements done to treat mitral stenosis?
- what are the two types of valves that can be used in an open heart mitral valve replacement?
- what are the pros and cons of each?
- done in mitral stenosis patients with exertional symptoms:
- valve replacements:
-
mechanical mitral valve:
- this valve has a longer lifepan than bioprosthetic valves
- these patients are given lifelong warfarin (comoudin) anticoagulant
-
bioprosthetic mitral valve:
- dont require anti-coagulants
- for patients 65 or older OR who cannot take anticoagulants
-
mechanical mitral valve:
complications of mitral stenosis
aka, the clinical manifestations of mitral stenosis. this list should be familiar.
- LA enlargement
- stroke/thrombus formation
- pulmonary hypertension
- right ventricular hypertrophy
- right sided heart failure
- peripheral edema
- JVD
- ascites
- hepatic congestion/cirrhosis
what is mitral regurgitation
the inability of the mitral valve to fully close, resulting in a backflow of blood int the left atrium
primary vs secondary mitral regurgitation
- Primary: resulting from detect of valve & its components
- Secondary: regurgitation resuling from progressive enlargement of LV that ends up causingcausing mitral annular dilation
what are the two types of non-infective endocarditis? what do they have in common?
- marantic endocarditis and libman sacks disease
- both involve sterile vegetations
- marantic endocarditis
- describe its vegetations
- effects what valves
- is associated with what underlying diseases/populations
- marantic endocarditis = a non-infective endocardtitis
- vegetations
- sterile
- small (1-5 mm)
- typically occur along the lines of closure
- are non-invasive: do NOT cause inflammatory response.
- mitral & aortic valve
-
associated w/ underlying systemic hypergoabulable state
- cancers patients, pts with catheters, sepsis, anti-phopholipid disorder
- can cause systemic emboli –> stroke
- vegetations
- libman sacks disease
- describe its vegetations
- what valves does it effects
- what underlying diseases/populations is it associated with?
- libman-sacks = a non-infective endocarditis
- vegetations
- small (1-4 mm)
- single or multiple sterile, pink vegetations
- warty appearance
- tend to extend into endocardium/chordae tendinae (not confined to closure lines like marantic*)
- tend to cause intense inflammation! (unlike marantic*)
- mitral & tricusupid valve
- associated with:
- SLE (systemic lupus erythematous): see in young females, causes strokes
- anti - phospholipid syndrome: seen mostly on aortic/mitral vavlve
- vegetations
what valvular disease is shown here?

marantic endocarditis (non-infective)
note the vegetations confined to the closure lines
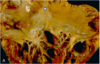
what valvular disease is shown here?

libman sacks disease (non-infective endocarditis)
note the pink, warty vegetations extending onto chordae tendinae/other valve components
physiological presentation of acute mitral regurgitation
- note the volume/pressure status of the heart chambers
- note cardiac ouput status
- regurgitation of blood from LV to LA during systole increases LA pressure and volume. since not all of LV blood is getting to the aorta, the end diastolic volume in the LV is decreased
-
increased LA volume and pressure
- can cause pulmonary edema
- decreased LV volume --> therefore low cardiac ouput
-
increased LA volume and pressure
discuss the physiological presentation of chronic mitral regurgitation
- note the volumes/pressures of the four heart chambers
- note the status of the cardiac ouput
- regurgitation of LV blood into LA during systole increases LA pressure/volume. over time, accumulated LA blood + new blood from venous return increases the point of also increasing end diastolic volume in LV.
- increased** LA volume and pressure**
-
increased LV volume and pressure
- cardiac output maintained

clinical presentation of acute mitral regurgitation
-
acutely ill and often in cardiogenic shock*
- due to low cardiac ouput unique to acute MR.
- this would be indicated by dyspnea, hypotension, tachycardia, cool extremities, diaphoresis
- chest pain
- acute pulmonary edema
clinical presentation of chronic mitral regurgitation
-
very similar to that of mitral stenosis due to LA volume “back up” the lung & right heart
- dyspnea
- peripheral edema
- JVD
- ascites
- palpitations/atrial fibrillation
- stroke
what are the key exam findings pertinent to mitral regurgitation?
- describe sounds heard on ascultation
- other clinical findings
- ascultation
-
sounds/mumurs:
- S1 decreased (soft mitral valve closure sound)
- S2 is split (delay between seminlunar valve closure)
- occasional S3 heard - would sound like kentucky
-
systolic murmur: created by blood flow thru mitral valve during sysole when it should be shut.
- holosystolic murmur in chronic MR
- early systolic murmur in acute M
-
possible laterally displaced PMI
- seen chronic MR, due to enlarged LV
-
sounds/mumurs:
- other exam findings
- may see signs of right heart failure - ascites, JVD
- may see signs of cardiogenic shock - hypotension, tachy, cold skin - if acute MR
- .discuss the systolic murmur heard in mitral regurgitation
- how is it different beween acute vs chronic MR?
- do we hear this in mitral stenosis?
- acute vs chronic MR:
- acute MR –> early systolic murmur
- chronic MR –> holosystolic murmur
- heard throughout systole (the whole time between S1-S2)
- radiates to the axilla
- do not hear a systolic murmur in mitral stenosis.
- in MS, the mitral valve closes sufficiently during systole but does not open sufficiently in diastole. thus, in MS we hear a diastolic murmur - created by turbulent blood flow during diastole
diagnostic testing for mitral regurgitation
- what is the “standard”? what are other useful tests and in what circumstances?
- compare/contrast this to dx of mitral stenosis
- like in mitral stenosis:
- echocardiogram is the diagnostic standard
- TTE - sufficient in most circumstances
- TEE - for detailed valvular anatomy/presence of thrombi
- EKG - if you suspect rhythm abnormality
- cardiac catheriziation - done if echocardiogram does not give definitive diagnosis
- echocardiogram is the diagnostic standard
- unlike mitral stenosis:
- consider chest x-ray to assess fluid overload/overall heart size
- don’t need to do an exertional test
how to treat severe acute mitral regurgitation
- most important: treat shock
- treat underlying cause of MR
- consider surgery
how to treat chronic asymptomatic MR
- control HTN
- medications: warfarin if a-fib present
- monitor w/ echocardiogram every 6-12 months
- consider surgical repair if:
- a-fib present
- of EF < 60% or LV end-diastolic volume of 4- mm
- pulmonary HTN present
how to treat chronic symptomatic mitral regurgitation?
-
just like with asymptomatic chronic MR:
- control HTN
- give warfarin if they have a-fib
- specific tx for primary vs secondary chronic symptomatic MR:
-
primary MR:
-
tx = valve surgery:
-
repair: open vs mitral cip
- mitral clip:
- not as effective as open
- but minimally invasive
- is thus good for high risk patients who cannot undergo open heart surgery as it can reduce symptoms enough to improve quality of life
- open alfari stitch repair
- mitral clip:
-
replacement: mechanical vs bioprosthetic valve (same as MS)
- recall that mechanical valves have a longer lifespan but require lifelong anti-coagulants
-
repair: open vs mitral cip
-
tx = valve surgery:
-
secondary MR:
-
no surgery
- since secondary MR is due to LV enlargement rather than a defect of the valve itself, repair/replacement does not fix the underlying problem
-
no surgery
-
primary MR:
what is mitral valve prolapse?
myxomatous degermation of the mitral valve that causes leafelets to bulge back into the left atrium
symptoms of mitral valve prolapse
- symptoms
- Palpitations
- Syncope
- Chest pain not associated with CAD
exam findings of mitral valve prolapse
- what will the ausculation show?
- other exam findings?
- what diagnostic test is standard to dx for mitral valve prolapse?
- ascultation:
- could show mid-systoic click followed by late-peaking systolic murmur
- other exam findings: typically normal unless MR (mitral regurgitation) is also present
- diagnostic standard: echocardiogram
- (like with all valvular diseases)
what is the treatment for mitral valve prolapse?
- typically no treatment unless MR is also present
- if there is treatment:
- possible beta-blockers - if palpitations
- baby aspirin - to reduce stroke risk
- if surgery:
- done when pt’s have severe MR symptoms
- men typically have surgery more (if someone)
triscuspid valve
- describe its anatomy
- where in the heart is it found
- when during the cardiac cycle is it typically open?
- what is its normal valvular area?
- three valves
- between RA and RV
- open during systole
- normal valvular area: 4-6 cm2
- describe the disease incidence of the tricuspid valve relative to the other valves
- what diseases most commonly effect the tricuspid valve and in what populations?
- lower incidence of disease than in aortic/mitral valves
- triscupid valve disease is most commonly seen IV drug users, and is usually one of the two:
- rheumatic heart disease
- infective endocarditis (IE)
tricuspid stenosis
- incidence
- causes
- incidence: rare
- causes:
- rheumatic heard disease - most common
- other causes:
- carcinoid heart disease
- myxoma/metastasis
- vegetations obstructing RV inflow
- typically from pacemaker leads
carcinoid heart disease
- cause
- pathogenesis
- gross presentation
- associated clinical presentaiton
- what markers aid in diagnosis of this cardinoid heart disease?
- cause/pathogenesis/presentations:
- cardinoid tumors (though, typically not GI carcinoid tumors)
-
bioactive products released from these these cardinoid tumors - serotonin (5-HT), kallikrein, bradykinin, histamine, prostaglandins - cause “carcinoid syndrome”- which can lead to the following:
-
clinical presentation:
- nausea/vomitting/diarrhea
- cramps
- episodic skin flushing
-
gross cardiac presentation:
- plaque-like thickening of the endocardium & valves of the heart. specifiaclly, the right heart valves- pulmonary & tricuspid
-
clinical presentation:
- markers:
- plasma levels of serotonin and 5-hydroindoleacetic acid (urinary serotonin) correlete to severity of the lesions
clinical presentation resulting from carcinoid heart disease
- symptomatology resulting from carcinoid heart disease is largely due to the increased systemic venous pressure resulting from increased right sided pressure
- peripheral edema
- abdominal distention
- RUQ pain/fullness
- neck pulsation
exam findings seen with carcinoid heart disease:
- auscultation
- other exam findings
-
right sided heart failure findings:
- JVD with cannon-a waves
- hepatomegaly
- ascites
- peripheral edema
- auscultation:
- murmurs:
-
low pitched diastolic mumur at the lower left sternal edge
- __due of turbulent flow thru tricuspid valve during diastole (tricuspid located at left lower sternal border) - all physicians take money
- increase with inspiration
- often heard alongside mitral stenosis murmurs
-
low pitched diastolic mumur at the lower left sternal edge
- murmurs:
what is mitral regurgitations and its primary causes?
- inability of the leafelets the fully close
- caused by same causes as carcinoid heart disease:
*
- what are the diagnostic tests to order for carcinoid heart disease and what key things will they show?
- echocardiogram - standard
- shows tricuspid valve pathology: thickened leafelets, decreased mobiliby, doming
- EKG:
-
possible peaked P-wave in lead II
- due to RA enlargement
- atrial fibrillation
-
possible peaked P-wave in lead II
- Chest X-ray:
- RA enlargement - seen as prominence of right heart border
what is the treatment regimen for carcinoid hear disease:
- first: relieve venous congestion
- use diruetics or nitrates (vasodilators)
- next: dubulk obstructive tumors/myoxomas in the heart
- consider the following:
- control a-fib
- anti-coagulants if needed
- surgical valve replacement:
- do if
- mean diastolic pressure gradient > 5mmHg & tricsupid orifice < 2.0 cm2
- or if concurrent mitral valve repair is happening
- do NOT do balloon valvoltomy
- do if
what is tricuspid valve regurgitation and its common causes?
- inability of valve leafelets to close
- causes:
- most are same as tricuspid stenosis/carcinoid heart disease:
- rheumatic heart disease
- IE
- myxomatous disease
- carcinoid heart
- could also be dilation due to –> pulmonary HTN –> putting pressure on RV –> RV overload opens trisupid valve
- most are same as tricuspid stenosis/carcinoid heart disease:
clinical presentation of tricuspid regurgitation
- Symptoms often associated with left sided heart disease or pulmonary disease
- Dyspnea
- Paroxysmal nocturnal dyspnea
- Peripheral edema
- Abdominal distension
- Peripheral edema
- Chest pain
exam findings for tricsupid regurgitation
- what will be seen on ascultation
- other findings
- ascultation:
- murmurs
-
low intensity holocystolic murmur:
- due to open tricsupid valve when it should be closed during systole
- heard at left sternal edge/subxiphoid area
- may hear S3
-
low intensity holocystolic murmur:
- murmurs
- prominent cv wave
- signs right sided heart failure
- JVD
- ascites
- hepatomegaly
- perpheral edema
treatment for tricuspid valve?
- medications
- treat HF with diuretics
- treat underlying cause (COPD, pulmonary HTN, ect)
- surgery:
-
surgical tricsupid annuloplasty is the go-to
- a “semi-prosthetic” ring
- valve replacement is rare
- but it if is, use bioprosthetic valve
- this is because a bioprosthetic valve doesnt require anti-coagulants, and the tricuspid valve is fairly prone to thrombosis
- but it if is, use bioprosthetic valve
-
surgical tricsupid annuloplasty is the go-to
