Maternal adaptations to pregnancy Flashcards
LO
- To explain the concept of ‘foetal autonomy’: how endocrine signals of placental origin alter maternal physiology
- To explain the alterations in the maternal cardiovascular, respiratory, and metabolic systems which optimise the delivery of oxygen and glucose to the foetus
- To examine how the mother’s response to the challenges of pregnancy may be influenced by the environment, with implications for later health of the offspring and the mother
What is required to grow a baby?

Why must maternal physiology change?
In order to provide for her baby and to provide for herself
How must her physiology change to provide for her baby?
There must be an increase in metabolism for oxygen and an increase in nutrients for glucose

How must the mothers physiology change to provide for herself?
prepare for metabolic demands of later in pregnancy (fat and protein deposition) - first trimester
prepare for delivery (reproductive tract) and feeding the baby (mammary glands) - later in pregnancy
Tell me the hormones that are involved in the foetal anatomy when they signal to the mother

How do the levels of the following hormones change over the course of gestation:
hCG
hPL
Progesterone
Estriol
Estrone
Estradiol

What are some physiology changes during pregnancy and why do each of those changes occur?
Cardiovascular changes
to supply extra blood to maternal tissues and to the uterine circulation
Renal changes
to achieve expansion of the blood volume and to remove metabolic waste products from the foetus
Respiratory changes
to supply extra oxygen for the increased metabolic demands of both mother and foetus
Metabolic changes
to provide for the mother’s needs and to supply nutrients for the growing foetus
Tell me the maternal cardiovascular adaptation and what this helps with
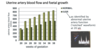
Increase in uterine artery blood flow aids nutrient delivery → increase foetal growth
How is this achieved? All about oestrogen
Uterine blood flow increases over the course of pregnancy: this aids foetal growth
This is supported by the graph on the right which shows foetal growth over the course of pregnancy

Oestrogen causes blood vessels to do what?
How does it do this?
Vasodilation
Increases the production of locally acting vasodilators e.g., nitric oxide (NO) and prostacyclin

What does vasodilation reduce?
Peripheral resistance
Peripheral vascular resistance (systemic vascular resistance, SVR) is the resistance in the circulatory system that is used to create blood pressure, the flow of blood and is also a component of cardiac function. When blood vessels constrict (vasoconstriction) this leads to an increase in SVR.

How is cardiac output affected during pregnancy?
What formula is used to show this?
Maternal cardiac output is increased
This adaptation is complete by mid-pregnancy
Cardiac output= blood being pumped out of heart at any one given time
CO= HR (heart rate) X SV (stroke volume- volume of blood being pumped during each heartbeat)

Tell me about how maternal systolic and diastolic BP is affected by pregnancy
decreases for most of pregnancy
- decrease in peripheral resistance
- expansion of placental circulation
slight increase to pre-pregnant levels 36 - 40 weeks
BP is monitored during pregnancy - for signs of pre-eclampsia
Decreases systolic and diastolic BP over course of pregnancy- slightly increases at end of pregnancy but never to normal levels
Preeclampsia is when BP gets very high and if left untreated it can lead to seizures and can be fatal

How is plasma volume and total body water volume affected during pregnancy?
They are both increased during pregnancy
Increases in blood volume during pregnancy and follows the same pattern as foetal weight gain
Risk of too much fluid in interstitial fluid- due to massive increase of water volume during pregnancy- risk of oedema

How is renal function affected during pregnancy?
The achieve maternal plasma volume expansion
1. Change in kidney function
2. Increased activity of the renin-angiotensin-aldosterone system (RAS)
- Regulate retention of sodium and water in kidney
3. Changes in blood osmolality (solute concentration)
- Fluid retention and regulation of thirst
How is the maternal kidney function affected during pregnancy?
Increased cardiac output increases renal blood flow
Glomerular filtration rate (GFR) increased by 40%-50%
Sodium and water excretion from the kidney function is regulated by the RAS (renal angiotensin system?)

How is the RAS influenced by pregnancy hormones?
Aldosterone from adrenal gland and this regulates sodium and water balance in the kidney
The hormones we see during pregnancy stimulate this whole pathway
Learn the pathway and how a high levels of oestrogen effects the hormonal output of the adrenal gland
All this increases blood volume and fluid retention during pregnancy
Progesterone has an opposite effect but all about balance between the two hormones
Angiotensin II is a vasoconstrictor

How is maternal haemodilution affected during pregnancy?
Maternal haemodilution
- Plasma volume increases more than red cell mass
Decreased haemoglobin concentration
- Risk on anaemia- not having enough iron or RBC during pregnancy

Tell me that changes that occur in osmoreceptor function
plasma solute concentration (osmolality) is about 10 mOsm/kg less than non-pregnant (more ‘dilute’ blood plasma)
normally, this would decrease anti-diuretic hormone (ADH) secretion to allow more fluid loss
however hypothalamic osmoreceptors have reduced threshold in pregnancy

What are the respiratory changes that occur in the mother during pregnancy?
supply of oxygen to maternal tissues must increase
oxygen transfer across the placenta to the foetus must be increased

How is the increased oxygen demand met?
No change in respiratory rate, vital capacity, or inspiratory reserve volume, but:
1. tidal volume increased by up to 40%: (tidal volume= breathing in and out)
deeper breathing, increased air flow resulting in increased O2 alveoli absorption
leads to decreased maternal [CO2]- changes metabolics of the mother
2. maternal pulmonary blood flow increase by 40% (due to increased CO)
per time, more blood available to absorb O2 across lungs
progesterone:
increases sensitivity to decreased [CO2]
causes dilation of airways to get more air into the lungs during pregnancy
3. increased red blood cells → increased O2 carrying capacity of the blood
4. Increased 2,3-diphosphoglycerate - an anion which displaces O2 from haemoglobin → more O2 release to tissues
5. foetal Hb has greater affinity for O2 than maternal Hb → enhanced placental O2 transfer

How is the maternal metabolism affected during pregnancy?
increase in maternal protein reserved, mothers own metabolism for growth of tissues that will be in use i.e., uterus, muscles and breast tissues towards end of breast feeding at end of birth
–> growth of uterus, musculature, and breast tissue
Early increased in maternal fat reserves- particularly in the first part of pregnancy
Energy store during first part of pregnancy and energy release during the latter part of pregnancy
Fatty acids important- maternal tissues become more insulin resistant in late pregnancy

Tell me about maternal insulin resistance during pregnancy
relative insulin resistance results in increase in circulating glucose levels in late pregnancy
- glucose promotes foetal growth
placenta produces anti-insulin factors
- hPL, placental growth hormone, oestrogen, and progesterone
gestational diabetes

What if adaptations are not optimal?
What might influence these adaptations?
Problems for mother and/or baby?
Metabolic:
maternal glucose supply
Cardiovascular (CV):
uterine artery blood flow
Placenta