Lecture 10: STEMI and NSTEMI Flashcards
(50 cards)
What is the underlying condition/ECG changes called if coronary flow is fully occluded vs. partial occlusion?
- Fully occluded = STEMI
- Partial = Unstable Angina or NSTEMI
Which type of MI is sympathetic hyperactivity (↑ HR, ↑ BP) vs. parasympathetic hyperactivity (↓ HR, ↓ BP) seen in?
- Sympathetic = anterior MI
- Parasympathetic = inferior MI
What are 4 PE findings associated with HF?
- S3
- Crackles
- ↑ JVD
- New murmur
Everything as far as presentation and ECG will be the same for NSTEMI and NSTE ACS, except for what?
NSTEMI will have elevated cardiac enzymes
Which cardiac conduction abnormality can obscure ST elevation analysis and may hide the manifestations of a STEMI?
New LBBB
Which ECG changes will be seen in the early acute phase of a STEMI?
- T wave increase in amplitude (like seen in hyperkalemia)
- Hyper-acute pattern
- Convex upward ST pattern

Besides STEMI, what are 3 other causes of ST segment elevation?
- Pericarditis
- LVH w/ J point elevation
- Normal variant (early repolarization) common in young males and african americans
If a patient with no chest pain and who seems normal has this ECG, what is one characteristic that tells you it’s likely not a STEMI?

- ST elevations are concave (if convex that would be early/acute MI)
- This is early repolarization a normal variant in young males

In the chronic phase following STEMI, if there is persistent ST elevation (after 2 weeks) what complication should you suspect?
LV aneurysm
Q waves shouldn’t be more than how many seconds in width?
No more than .03 sec in width
Which lead is the T wave normally inverted and may be variable in which?
- Inverted in aVR
- Variable in lead III
Which waves/segments of the ECG represent ischemic pattern, injury pattern, and pattern of necrosis/infarction?
- Ischemia –> impaired repolarization –> T waves changes (inverted/tall/peaked)
- Injury –> inability to fully polarize –> ST elevations
- Infarction/necrosis –> lacks depolarization –> Q wave or QS complex

Since there are no posterior leads, how do we view a posterior wall infarction and look for what?
- Look at V1-V3 (anterior leads) and will be a mirror image
- So looking for ST depression and a prominent R
After several weeks or months following an MI what Q, R, T and ST changes will exist?
- Significant Q wave usually persists
- Some R wave may return
- T wave often less inverted
- ST elevation may persist IF aneurysm develops

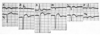
What does this ECG signify and how can you tell?

- Recent MI of LAD (leads V1-V6)
- Massive Q waves + T wave inversion + ST elevation
What is your interpretation of this ECG?
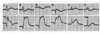
STEMI - Anterior Wall (LAD)

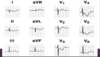
What is the ECG indicative of?

- Anterior wall STEMI w/ left anterior hemiblock
- The L.A.D and small R waves in II, III, and aVF meet criteria for left anterior hemiblock

Patient presents with what appears to be an MI and this is his ECG, where is the infarction and why?

- TRUE Posterior infarct
- Based on the reciprocal changes in anterior leads;
- V1 shows large R (reciprocal of posterior Q) and upright T wave (reciprocal of posterior T inversion)

What type of MI is this indicative of?

Posterior wall infarction

Pt presents w/ chest pain and what looks do be an MI, this is his ECG, what do you suspect?
NSTEMI or NSTE ACS
*Need enzymes*

Failure of which organ can give false positive elevations of Troponin T (CTnT)?
Renal failure, since is excreted by kidneys
For patient with acute STEMI what are the reperfusion strategies if hospital has cath lab and how soon?
- Primary percuteanous coronoary intervention (PCI) w/ angioplasty and stenting
- Cath lab within 90 minutes (goal)
If hospital does not have cath lab or there isn’t time to get to one what is done for acute STEMI and how quickly?
- Give fibrinolytic or thrombolytic
- Begun in ED within 30 mins. (goal)
After beginning fibrinolysis therapy in pt with acute STEMI if there is failure of ST elevation to resolve by >50-70% within 1-2 hours this suggests what?
Failure of fibrinolysis


