What are the pre-requisites for IOL?
- able to perform CS if necessary
- maternal
- ripe cervix, open os
- if cervix not ripe, use prostaglandin vaginal insert (cervidill)
- fetal
- normal fetal heart trace
- cephalic presentation
- adequate fetal monitoring available
- maternal
- likelihood of success determined by Bishop score (>6 favourable)
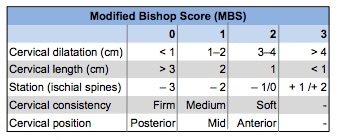
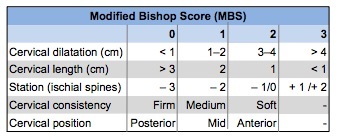
What is the Bishops score?
- Position
- Consistency
- Effacement
- Dilation
- Station
- Favourable cervix = >6
- score 9-13 = high likelihood of vaginal delivery
What methods are there for IOL? How do you decide which one to use?
- balloon catheter
- ARM
- dinoprostone
- oxytocin
Based on:
- membranes ruptured?
- yes = oxytocin
- no = check bishop score
- cervix favourable?
- yes = ARM
- no = balloon catheter OR dinoprostone
- no + previous CS = balloon catheter only
What are the indications for balloon catheter?
- Indications
- MBS ≤ 6
- Previous CS
- Following dinoprostone if no/minimal effect on cervical ripening and ARM not technically possible
- Reduced risk of uterine hyperstimulation is desirable
Contraindications for balloon catheter?
- Contraindications
- Ruptured membranes
- Undiagnosed bleeding
- Simultaneous use of prostaglandins
- Low lying placenta
- Polyhydramnios
- Abnormal FHR auscultation or CTG
- Relative contraindications
- Antepartum bleeding
- Lower tract genital infection
- Fetal head not engaged
How much longer after balloon catheter is inserted does it need to be reviewed?
- 12 hours
- DO NOT LEAVE IN FOR >18HRS
- if no SROM recommend ARM
What are the indications for dinoprostone?
Prostaglandin E2
Indications
- Unfavourable cervix (MBS ≤ 6)
- Following balloon catheter if no/ minimal effect on cervical ripening and ARM not technically possible
What are contraindications to prostaglandin E2?
Contraindications
- Known hypersensitivity
- Ruptured membranes
- Multiparity ≥ 5
- Previous CS or uterine surgery
- Malpresentation/high presenting part
- Undiagnosed PV bleeding
- Abnormal CTG/fetal compromise
What should you be cautious of when using prostaglandin E2?
Cautions
- Multiple pregnancy
- Asthma, chronic obstructive pulmonary disease: may cause bronchospasm
- Epilepsy
- Cardiovascular disease
- Raised intraocular pressure, glaucoma
- Avoid concurrent oxytocin use
When should you review prostaglandin E2 lady?
- gel = 6 hours
- pessery = 12 hours
Then recommend ARM regardless of MBS
Indications for ARM?
Indications
- After cervical ripening method
- Favourable cervix (MBS ≥ 7)
- Before oxytocin infusion commenced
Relative contraindications of ARM?
Relative contraindications
- Poor application of the presenting part/unstable lie
- Fetal head not engaged
Inducing a lady for labour. Need to do a vaginal exam. What do you assess?
VE to identify:
- Stage of labour
- MBS
- consistency
- effacement
- position
- dilation
- station
- Presentation
- Position and descent
- Membranes
What clinical concerns do you need to assess for when thinking about performing an ARM?
- Polyhydramnios
- Head not engaged
- Malpresentation
- Possible cord presentation
- Unstable lie
if any of the above, consult obstetrician
What do you need to check for AFTER performing ARM?
- fetal heart rate
- liquor abnormality
if nil, commence oxytocin !!!!!
Indications for oxytocin in IOL?
Indications
- IOL with ruptured membranes
What do you need to be cautious of when giving oxytocin?
- Do not commence oxytocin within:
- 6 hours of dinoprostone gel
- 30 minutes of removal of dinoprostone pessary
- Discuss with obstetrician if:
- Previous uterine surgery (e.g. CS)
- Multiple pregnancy
- More than 4 previous births
- Cardiovascular disease
What are the potential side effects of oxytocin?
- Uterine hyperstimulation
- Nausea and vomiting
- Water intoxication or hyponatremia with prolonged infusion (rare with isotonic infusion)
- Primary postpartum haemorrhage
- If planned VBAC: uterine dehiscence and rupture
- Rarely (< 0.1%) arrhythmias, ECG changes, anaphylaxis, tetanic contractions, transient hypotension, reflex tachycardia
What kind of contractions are you aiming for when giving oxytocin?
Aim for contractions:
- 3–4 in a 10 minute period
- Duration of 40–60 seconds
- Resting period not less than 60 seconds
For uncomplicated pregnancies, when should you recommend IOL?
41 weeks
Why should you induce at 41 weeks as compared to expactant management in an uncomplicated pregnancy?
IOL from 41+0 weeks, compared with expectant management, is associated with:
- Fewer perinatal deaths [0.4 versus 3.2 per 1000 women]
- Less meconium aspiration syndrome [40 versus 66 per 1000 newborns]
- No difference in neonatal intensive care (NICU) admissions
- Fewer caesarean sections (CS) [168 versus 225 per 1000 women]
- Most women prefer IOL at 41 weeks over serial antenatal monitoring
For women >40 years old, when should you suggest IOL?
39-40 weeks
When should you induce a lady who’s baby has fetal macrosomia?
Discuss IOL after 38+0 weeks if EFW greater than:
- 3.5kg at approximately 36 weeks
- 3.7kg at approximately 37 weeks
- 3.9kg at approximately 38 weeks
What do you need to do in your assessment immeadiately before IOL?
- Immediately prior to IOL:
- Review maternal history
- Confirm gestation
- Perform baseline maternal observations (e.g. temperature pulse, respiratory rate and blood pressure)
- Perform abdominal palpation to confirm presentation, attitude, lie, position, and engagement
- Assess membrane status (ruptured or intact)
- Vaginal examination (VE) to assess the cervix
- Assess fetal wellbeing:
- FHR
- Confirm CTG is normal
- If CTG abnormal, escalate as per local protocols
- Assess for contraindications to IOL
- consider urgency of IOL
