Inflammatory Myopathies and Polyarthragia Rheumatica Flashcards
(62 cards)
What drugs may induce symptoms that mimick Myositis disorders?
- HMG-CoA reducatase inhibitors => statins
- Note: these drugs may even lead to the formation of antibodies that bind HMG-COA reductase
ALSO, proliferating muscle has been shown to express HMG-CoA reductase, this may be why antibodies against HMG-CoA reductase cause RHABDOMYOLYSIS
What pattern of muscle involvment do you expect to see in inflammatory myopathies?
•what muscles are affected (generally)?
Mostly striated (skeletal) muscles are affected in Dermatomyositis and Polymyositis. Muscle involvment in these diseases is typically symmetric and PROXIMAL.
Specifically, what muscles often become weak in myositis?
• Neck
• Abdominal Mm.
• Upper 1/3 of Esophagus
• Diaphragm/Thoracic Muscles
• Problems with sphincter ani causing urinary incontinence.
What is the major differentiating factor between polymyositis and dermatomyositis?
• SKIN INVOLVMENT
Aside from diaphragmatic weakness, what pulmonary complications should patients with Polymyositis and Dermatomyositis be warned of?
70% of patients may present with interstitial lung disease of varying degrees but still very similar to ideopathic interstitial lung disease (remember this dz? honeycomb lung, 3-5 yrs to live, pattern of involvment from exterior of lung towards the inside)
***Clearly this is a bad px***
What symptoms should you start looking for in a patient with Polymyositis or Dermatomyositis that is positive for anti-Jo-1 antibodies?
• what are anti-Jo-1 antibodies directed against?
• What is this called?
• How often is this seen?
Arthritis and Mechanics Hands are associated with myositis that is accompanied by anti-Jo-1 antibodies, this is called ANTISYNTHETASE SYNDROME. 20% of patients with DERMATO- or POLYMYOSITIS will have this.
• Abs. Directed against histidyl-tRNA synthetase (and other anti-synthetase abs are associated with the developement of arthritis as well)
Is the heart involved in Polymyositis and Dermatomyositis?
• Yes you can see heart involvment with conduction abnormalities, and arrythmias, myocarditis, and CAD.
What is a common GI complaint of someone with a myositis?
Difficulty swallowing
Note: GI problems in patients are most commonly related to weakness of the tongue, pharyngeal muscles, and sometimes lower esophagus, diarrhea, constipation, stomach pain all secondary to disturbed motility.Vasculitisof GI vessels resulting in bleeding can happen but israre.
Note: GI problems in patients are most commonly related to weakness of the tongue, pharyngeal muscles, and sometimes lower esophagus, diarrhea, constipation, stomach pain all secondary to disturbed motility. Vasculitis of GI vessels resulting in bleeding can happen but is rare.
Aside from dermatomyositis and polymyositis, what are 4 other types of inflammatory myopathies?
• Antisynthetase Syndrome (anti-Jo-1 antibodies)
• Amyopathic Dermatomyositis
• Juvenile Dermatomyositis
• Inclusion Body Myositis
Differentialte dermatomyositis and Amyopathic Dermatomyositis?
• What are some complications of amyopathic dermatomyositis?
Amyopathic Dermatomyositis is dermatomyositis without the myositis. Clearly these people are at a high risk of developing dermatomyositis especially later in dz.
RISKS:
• HIGH risk of IPF (interstitial pulmonary fibrosis)
****Because this disease often goes undiagnosed IPF is typically in late (honeycomb) stages before anyone catches it*****
What changes are seen in the joints of someone with antisynthetase syndrome?
- These patients get symmetric polyarthritis of small joints
- This arthritis is NON-EROSIVE (imp for ddx with RA)
What age groups experience the highest incidence of Juvenile Dermatomyositis?
• what additional features are seen in this disease that are not seen in the adult form?
Highest Incidence between 6 and 11 years old. These kids have all the same symptoms of adult dermatomyositis.
30-70% have additional symptoms of:
• Calcinosis
• Cutaneous Ulceration
• Lipodystrophy (calcification of fat)
What are the KEY features of inclusion body myositis?
• who presents with this disease and how do they present?
• what should you key in on when taking history?
• what can you tell this pt. about there outcome after treatment is initiated?
IBM (inclusion body myositis) typically presents with a 50 year old man with an insideous onset of muscle weakness (months -> years) that is localized primarily to his thigh muscles and fingers.
Inclusion body myositis can be familial or sporadic so he may have a positive family history of this disease.
We can give this guy glucocorticoids but it probably won’t do much for him.
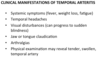
The following pictures are symptoms of what disease?
• name what you see in each picture.

DERMATOMYOSITIS is shown
A. Gottron’s Papules
B. Heliotrope rash
C. Gottron’s Sign on the knee
D. Gottron’s Sign on the elbow
Lupus involves the formation of a heliotrope rash as well as rashes on the hands etc. On the basis of physical findings alone how can you differentiate dermatomyositis from lupus?
A key difference is the pattern of the rash seen on the hands:
• in Dermatomyositis Redness overlies JOINTS
• in Lupus Redness SKIPS JOINTS

What is shown here?

Evidence of Capillary damage near the nailbed is a common feature of this disease is Raynaud’s which when severe enough may cause damage in the capillary beds
Name each of these signs associated with Dermatomyositis.
• what antibodies are likely to be positive on this person’s panel?

A. Linear Erythema
B. Scalp Rash
C. V-like sign
D. Shawl Sign
A, C, D are all associated with Anti-Mi-2 antibodies diffectes against nuclear helicase

A guy that is 55 y.o. presents to you with a history that includes increasing hip and shoulder pain. No cutaneous abnormalities are noticed on physical exam. He shows you his hands and they look like the picture shown below.
• What might this guy have?
• How could you nail down the dx?

Looks like this guy has polymyositis accompanied by Anti-synthetase syndrome which is why he is presenting with mechanic’s hands. Anti-Jo-1 antibodies would help assure you that this is PM + Anti-synthetase syndrome

Differentiate Polymyositis, Dermatomyositis, and Inclusion body myositis with respect to the patient that’s likely to present with it.
Polymyositis:
• is typically seen in females in their LATE teen or older with average age of onset being 50-60 y/o.
Dermatomyositis:
• BIMODAL with females 5-15 or 45-65 being most likey to get this disease.
Inclusion Body Dermatitis:
• Almost always 50 and up and is more common in males.
Do inflammatory myopathies ever occur in the setting of other autoimmune diseases?
YES, 11-40% of patients with other autoimmune diseases with get one. Typically htose with Connective Tissue autoimmune diseases are at the highest risk.
(e.g. systemic sclerosis, SLE, RA, Sjorgren’s, polyarteritis nodosa, Sarcoidosis)
A 59 year old woman presents to your office with Gottron’s nodules on her hands and a shawl rash. She has had increasing fatigue and has experienced stiffness in her shoulder and hip.
• What is the likely diagnosis?
• What should you do immediately after making this diagnosis?
This woman has Dermatomyositis. You should send her for cancer screens because 12% of patients with myositis present with cancer (typically breast adenocarcinoma) in the 1st year of diagnosis.
81% of the time the myositis is DM, the other 19% if PM
What conditions might you suspect if patients are positive for the following antibodies on their panel:
• anti-tRNA synthetases
• anti-Mi-2
Anti-tRNA synthetase abs.:
• Interstitial lung diseases
Anti-Mi-2 abs. (anti-nuclear helicase):
• Gottron’s Papules
• V sign
• Shawl sign
What are PM-scl antibodies associated with?
• features of this disease?
PM-scl antibodies are frequently associated with a POLYMYOSITIS (PM) - SCLERODERMA (Scl) cross over syndrome characterized by:
- mild muscle disease
- Prominent Arthritis
- Limited Skin Sclerosis
***Responsive to therapy***