Hypertension Flashcards
Normal BP
less than 120
and
Less than 80

Elevated BP
120 - 129
and
Less than 80

Stage 1 Hypertension
High Blood Pressure
130 - 139
or
80 - 89

Stage 2 hypertension
High blood pressure
140 or higher
or
90 or higher
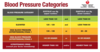
Hypertensive Crisis
Consult your doctor immediately
Higher than 180
and/or
Higher than 120

What is primary (or essential) hypertension
Primary (or essential) hypertension (90-95%): unclear etiology but multifactorial (genetic and environmental factors)
Recall that secondary hypertension (5-10%) is hypertension contributing to another disease or medications
What are the complications of hypertension
Left ventricular hypertrophy
Heart failure
ischemic stroke
Intracerebral hemorrhage
Ischemic heart disease
Chronic kidney disease and end-stage renal disease (bad for kidneys)
Risk of CVD doubles with every 20 mmHg increase, starting at 115 mmHg
Treatment of hypertension
address secondary cause, if present
lifestyle modification
Pharmacological therapy
What are first-line hypertension drugs?
What are different drug classes associated with hypertension drugs?
- roughly equivalent BP lowering efficacy
- Consider: cost, side effects, other health conditions, occasionally ethnicity
- Drug classes
- Thiazide diuretic
- Angiotensin-converting enzyme inhibitor (ACEI)
- Angiotensin II receptor blocker (ARB)
- Long-acting calcium channel blocker (most often dihydropyridines (DHP))
Understand the physiological mechanisms that can be targeted for the treatment of hypertension
Lifestyle Modifications
Weight reduction
Adopt DASH eating plan
Dietary sodium reduction
Physical activity
Moderation of alcohol consumption
Antihypertensives
Reduce sympathetic tone/stimulation
Beta-blockers (propranolol), alpha blockers (prazosin), alpha two agonist (clonidine)
- Antihypertensives; reduce plasma volume: diuretics
- gets rid of more fluid and therefore decrease blood volume
- Relax arterial smooth muscle, cause vasodilation (smooth muscle tone)
- Renin-angiotensin inhibitors
- Ca2+ channel blockers
What does Short term MAP regulation look like?
Depends on increases in CO and TPR through baroreceptor reflexes and SNS activation

What does Long-term MAP regulation look like?
vasoconstriction due to angiotensin II, increased fluid volume due to aldosterone and vasopressin

MAP =
CO x TRP
Beta-blockers = decrease in force and rate of cardiac contraction = decrease CO
Diuretics, angiotensin inhibitors, beta receptor blockers = Decrease blood volume = decrease CO
Peripherally acting sympatholytics, Ca channel blockers, direct vasodilators, angiotensin inhibitors = relax vascular smooth muscle = decrease TPR
Centrally acting sympatholytics, Beta receptor blockers -> decreased sympathetic outflow = decrease CO and TPR

Diuretics (“water pills”)
- Often a first choice for treatment of mild/moderate hypertension
- Low-cost but effective drugs: treatment of hypertension associated with reduced morbidity and mortality
- Act on various segments of the nephron to produce an increase in renal sodium excretion leading to an increase in urine volume

What are the initial and delayed effects of diuretics (“water pills”)
Initial effects: reduction in blood volume resulting in decreased blood pressure due to decreases in cardiac output (stroke volume)
Delayed effects: after 6-8 weeks, blood volume and cardiac output are restored back to normal, but peripheral resistance declines

What are mediators in secretion and reabsorption?
Within the kidney tubules
Tubular epithelial cells
Luminal membrane facing tubule lumen
Basolateral membrane near capillaries
Tight junctions
Membranes on both sides contain channels and transporters that move solutes
Reabsorption is regulated by transporters, not through the cells because the tight junctions block

Explain sodium Reabsorption
Two Steps
- Diffuses from lumen into epithelial cells
- Actively transported out of cell on basolateral side
Specific channels and transporters on luminal side differ in different regions of the tubules, but pattern remains the same

Furosemide
(Lasix)
Loop diuretics
Ethacrynic acid (edecrin)
Block Na/K/2CL cotransporter (NKCC2) in ascending limb of loop of henle
Na continues through the lumen of the nephron and reaches the collecting duct. More water is retained in the lumen due to the osmotic effect of Na+
Most common uses: edema; short-term management of severe hypertension
Highest efficacy of the diuretics

What is the highest efficacy of the diuretics
Furosemide
Loop diuretic
What are the major side effects of furosemide?
Hypokalemia (low potassium)
- K+ reabsorption decreased in loop
- K+ secretion in collecting duct is increased due to higher level of Na+ in the lumen
hydrochlorothiazide
Thiazide diuretics
Hydrochlorothiazide, chlorthalidone
Block Na/Cl cotransporter (NCC) in distal tubule
Major use: long-term outpatient management of hypertension
Efficacy to cause diuresis is lower than loop diuretics

What are the adverse effects of Thiazide diuretics (hydrochlorothiazide, chlorthalidone)?
Adverse effects: similar to loop diuretics, can cause hypokalemia due to higher levels of sodium in the collecting duct
Chlorthalidone is more efficacious and longer acting than* *hctz* but also carries *greater* *risk of hypokalemia

Diuresis caused by loop diuretics is _____________ that caused by thiazides
Diuresis caused by loop diuretics is greater than that caused by thiazides
Higher effect for loop diuretics vs. thiazide
- Max NaCl loop diuretics of the total amount 20-25% can be trapped in loop
- Thiazide max about 5
Loop of Henle has higher effect on the NaCl reabsorption

Potassium-sparing diuretics
- Work on principal cells of the cortical collecting duct
- Same region that is sensitive to aldosterone
- Sodium channels that is just a sodium channel that pumps in and out, in addition, there is a potassium only channel
- For loop diuretics. they cause hypokalemia because of the K loss

What are the 2 mechanisms of Potassium-sparing diuretics
2 possible mechanisms
- Block collecting duct Na+ channels amiloride, triamterene
- Block aldosterone receptor spironolactone, eplerenone
- The antagonist of the mineralocorticoid receptor and therefore opposite/blocking aldosterone

What drug block collecting duct Na+ channels?
in potassium-sparing diuretics
amiloride, triamterene

What drug blocks aldosterone receptors in potassium-sparing diuretics?
Spironolactone, eplerenone

What are the side effects unique to spironolactone?
anti-androgen effects including gynecomastia, impotence

Why are they called potassium-sparing?
Blocks Na reabsorption and therefore gets rid of less K
- In the collecting ducts, Na+ and K+ move in opposite directions
- Less Na+ reabsorbed = less K+ excreted
- K+ is “spared” ie maintained in the body

What are the major uses for potassium-sparing drugs?
Major uses: relatively weak as individual agents, however they:
- Can be useful in treating some cases of resistant hypertension
- Can offset hypokalemia caused by loop diuretics and thiazides

What are the adverse effects of potassium-sparing drugs?
Can lead to hyperkalemia - elevated K+

Renin-angiotensin related drugs result in what?
Aldosterone is released from the adrenal gland as a result of the:
Renin-Angiotensin Systems
SNS stimulation causes renin release from the kidney
Leads to angiotensin and aldosterone production
(vasoconstriction, Na and H2O retention = increase BP)

Drugs targeting the renin-angiotensin system are what? what do they specifically target?
Drugs targeting the renin-angiotensin system
- Direct renin inhibitor: aliskiren (not used much)
- ACE inhibitors: lisinopril
- prevent angiotensin II
- Angiotensin receptor blockers: losartan
- newer drug
NOTE: drugs affecting the RAS have been observed to be less effecting in black patients

Which drug is a direct renin inhibitor?
aliskiren
Targets the renin-angiotensin system

Which drug is an ACE inhibitor?
Lisinopril
Prevents angiotensin II
Renin-angiotensin system target

Which drug is an angiotensin receptor blocker?
losartan
Targets renin-angiotensin system

What are the ACE inhibitor-specific effects?
-
Another function of ACE is to break down bradykinin
- Bradykinin = inflammatory mediator that causes BV to dilate/increase permeability/edema
- Increased levels of bradykinin lead to dry cough as side effect in up to 20% of patients
- Less common but more serious: angioedema
- Swelling of tongue and aroudn eyes

What do calcium channel blockers do?
Calcium Channel Blockers
-
Lower BP by relaxing vascular smooth muscle
- decrease amount of Ca that can enter the cell and therefore decrease the smooth muscle contraction

Amlodipine
Dihydropyridines
Calcium channel blockers
Fairly selective for blood vessels - Ca channels in blood vessels

Verapamil
Non-Dihydropyridines
Also blocks cardiac calcium channels (in addition to vascular affects)
Decreases rate, contractility, oxygen demand
Useful if hypertension accompanied by angina or certain types of arrhythmias

Explain the mechanism for smooth muscle contraction
Arteriole smooth muscle contraction
Muscle contraction requires Ca2+ influx and/or release from the sarcoplasmic reticulum
