HISTO: Lung pathology Flashcards
List 4 common airway diseases.
(1) Asthma
(2) COPD – Chronic Bronchitis
(3) Bronchiectasis
(4) Infections
Define asthma. List some causes.
Widespread reversible narrowing of the airways that changes in severity over short periods of time.
Causes:
- Allergens/atopy
- Pollution
- Drugs (NSAIDs)
- Occupational (gases)
- Diet
- Physical exertion
- Intrinsic
- Genetics
Describe the pathophysiology of asthma.

Whata are the macroscopic features of asthma?

What are the histological features of asthma?
- Hyperaemia
- Eosinophilic inflammation and goblet cell hyperplasia - mucus
- Hypertrophic constricted muscle
- Mucus plugging and inflammation

Define COPD/chronic bronchitis. What are the causes?
COPD is chronic injury to airways elicits local inflammation and reactive changes
Definition = chronic cough productive of sputum; most days for ≥3 months over ≥2 consecutive years
Causes = smoking, air pollution, occupational exposures
What are the histopathological features of CODP?

What are the complications of CODP/chronic bronchitis?

Define bronchiectasis. What are the most common causes?
Bronchiectasis – permanent abnormal dilatation of the terminal bronchi
Causes:
- Congenital (CF, ciliary dyskinesia [i.e. Kartagener’s syndrome])
- Inflammatory (post-infectious, obstruction, 2nd to bronchiolar disease and interstitial fibrosis, asthma)
What are the complications of bronchiectasis?
RHF - cor pulmonale

How common is CF?
1 in 2,500 but 1 in 20 are carriers (heterozygous carriers as it is recessive)
What is the aetiology of CF?
Chr 7q3 = CFTR gene (ion transporter protein)–> defective Cl- ion transfer so less water transfer to secretions
Affects all organs (from abnormally thick secretions):
What are the complications of CF? What are the most common infections?
- Lung –> obstruction, respiratory failure, recurrent infection**, **bronchiectasis (90%), etc.
- S. aureus H. influenzae
- P. aeruginosa B. cepacia
- GI tract - meconium ileus, malabsorption
- Pancreas - pancreatitis, 2nd malabsorption
- Liver - cirrhosis
- Male infertility - blockage of sperm ducts
What is the management of CF? What is the prognosis?
Imrpoved treatment with PT, antibiotics, enzyme supplements, parenteral nutrition
Survival to 4th decade
Increased with lung transplantation
List 5 common parenchymal diseases.
(1) Pulmonary oedema and diffuse alveolar damage (include acute resp. distress syndrome and HMD)
(2) Infections
(3) COPD – emphysema
(4) Granulomatous diseases
(5) Fibrosing interstitial lung disease and occupational lung disease
Define pulmonary oedema. What are the causes?
= fluid accumulation in alveolar spaces
- Causes – LHF, alveolar injury, neurogenic, high altitude
-
Pathology:
- Intra-alveolar fluid on histology (left)
- “Heart failure cells” = iron-laden macrophages (right)

What is seen on histopathology of pulmonary oedema?
- Intra-alveolar fluid on histology (left)
- “Heart failure cells” = iron-laden macrophages (right)

Define alveolar damage. What is the pathogenesis?
Pattern of acute diffuse lung injury in which patient present with rapid onset respiratory failure, requiring ventilation on ITU. CXR shown “white out” of all lung fields.
Pathogenesis: Acute damage to endothelium ± alveolar epithelium leading to an exudative inflammatory reaction
What are the causes of alveolar damage such as ARS and hyaline membrane disease?
-
Adults = acute respiratory distress syndrome / ARDS
- Infection
- Aspiration
- Trauma
- Inhaled irritant
- Shock
- Blood transfusion
- DIC
- Drug overdose
- Pancreatitis
-
Neonates = hyaline membrane disease of the newborn / RDS (HMD of newborn = RDS)
- Insufficient surfactant
- Premature babies
What is the prognosis of diffuse alveolar damage?

What is the gross pathology of diffuse alveolar damage (DAD)?
- Fluffy white infiltrates in all lung fields
- Lungs expanded/firm
- Plum-coloured lungs, airless
- >1kg mass

What is the micropathology of DAD?
- Capillary congestion
- Exudative phase
- Hyaline membranes
- Organising phase

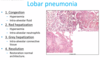
What are the patterns of baterial pneumonia?
- Bronchopneumonia
- Lobar pneumonia - aggressive phase, not seen as much
- Abscess formation
- Granulomatous inflammation
Describe the difference between bronchopneumonia and lobar pneumonia.