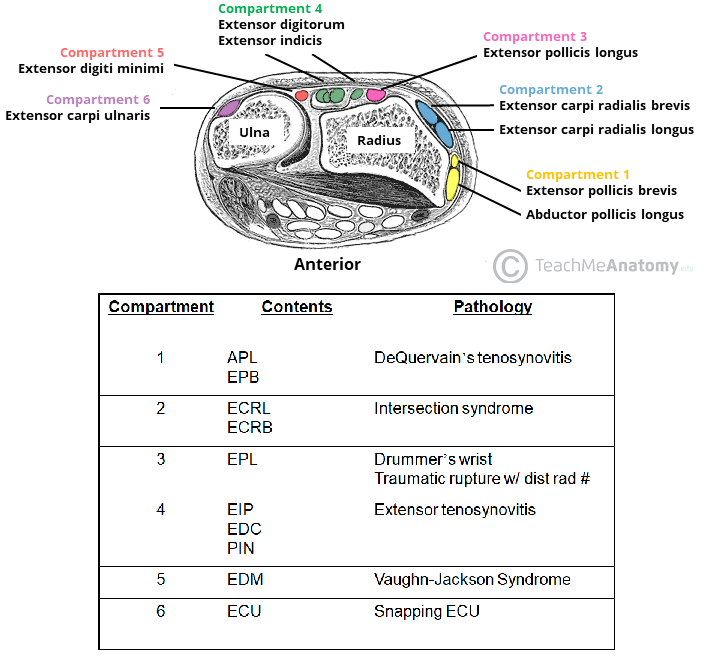
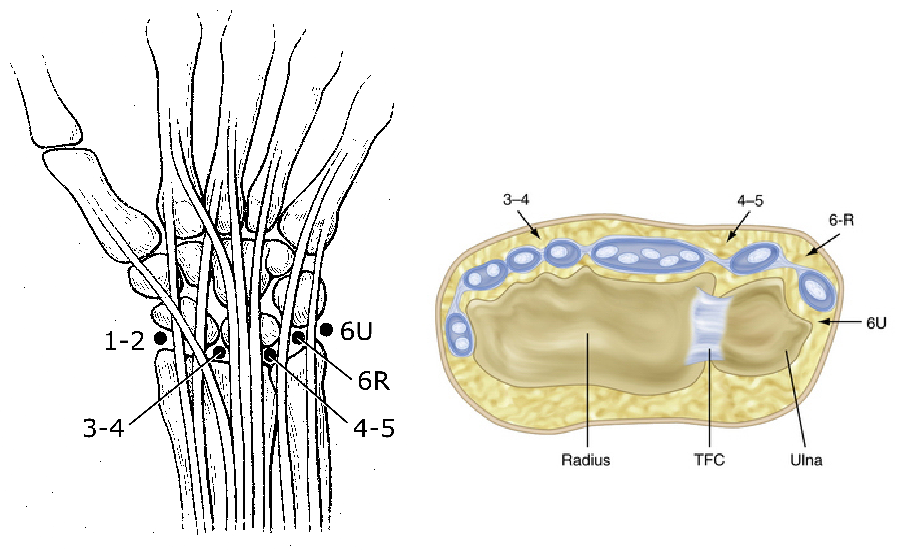
What are the extensor compartments of the wrist and associated pathology?
- EPB + APL = De Quervain’s tenosynovitis
- ECRB + ECRL = intersection syndrome
- EPL = drummer’s wrist, traumatic rupture with DR #
- EDC + extensor indicis = extensor tenosynovitis
- EDM = Vaughn-Jackson syndrome
- ECU = snapping ECU
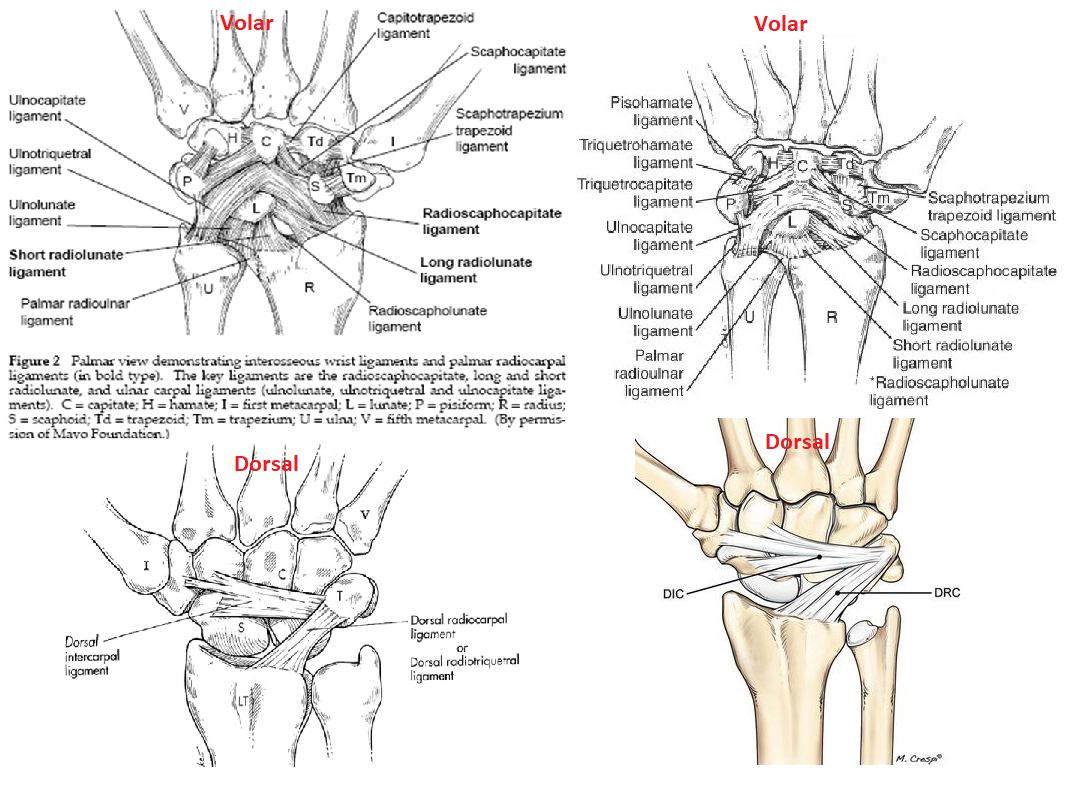
What are the extrinsic ligaments of the wrist?
[Rockwood and Green 8th ed. 2015]
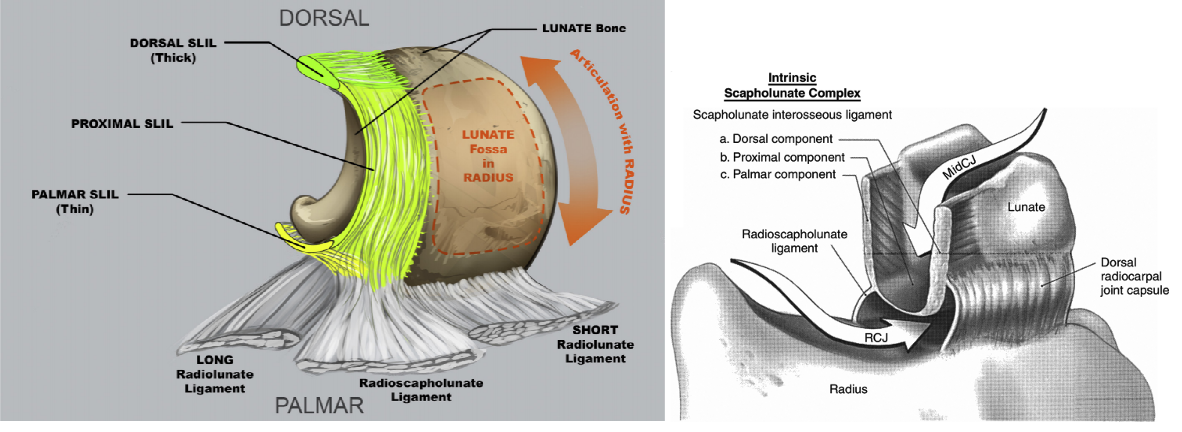
- Volar ligaments (radial to ulnar)
- Radial collateral ligament
- Radioscaphocapitate
- Radioscapholunate
- AKA Ligament of Testut
- Actually a n.v. bundle
- No contribution to carpal stability
- Long radiolunate ligament
- Short radiolunate ligament
- Ulnolunate ligament
- Ulnotriquetral ligament
- Ulnocapitate ligament
2. Dorsal ligaments - Dorsal radiocarpal ligament (DRC)
- Dorsal intercarpal ligament (DIC)
What is normal wrist ROM?
[JBJS REVIEWS 2015;3(1):e1]
- Flexion = 80o
- Extension = 70o
- Pronation = 90o
- Supination = 90o
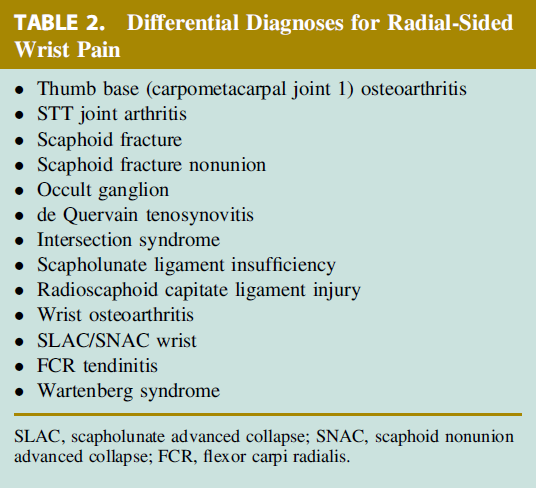
What is the differential diagnosis for radial sided wrist pain?
- Soft tissue
- De Quervains tenosynovitis
- FCR tendonitis/rupture
- Bone
- Radial styloid fracture
- Scaphoid fracture
- Joint
- CMC joint arthritis
- Radio-scaphoid arthritis
- Scapholunate instability
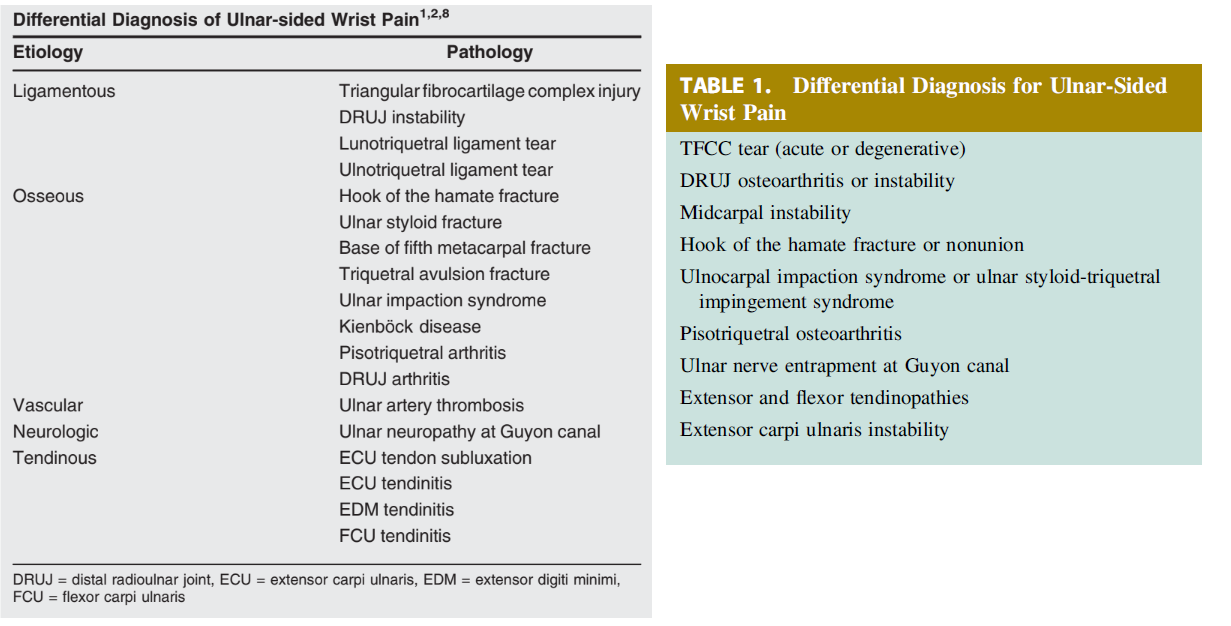
What is the differential diagnosis for ulnar sided wrist pain?
[JAAOS 2017;25:e150-e156]
- Soft tissue
- Snapping ECU/ECU tendonitis
- EDM tendinitis
- FCU tendinitis
- Bone
- Pisiform fracture
- Triquetral fracture
- Hamate fracture
- Ulnar styloid fracture
- Base of 5th metacarpal fracture
- Kienbock disease
3. Joint - Ulnar impaction syndrome
- Ulnar styloid triquetral impaction (USTI)
- TFCC tear
- Triquetrolunate instability
- Pisotriquetral arthritis
- DRUJ arthritis
- DRUJ instability
- LT ligament tear
- Ulnotriquetral ligament tear
4. Vascular - Ulnar artery thrombosis
5. Neurologic - Ulnar tunnel syndrome
Describe the SL ligament?
[JAAOS 2015;23:691-703]
Intra-articular C-shaped ligament with 3 components
- Dorsal – thickest, primary stabilizer
- Volar
- Proximal - thin, membranous
What is the motion of the scaphoid from ulnar to radial deviation ?
[JAAOS 2015;23:691-703]
Position of flexion and radial deviation to extension and ulnar deviation
What wrist motion minimizes motion between the scaphoid and lunate and minimizes tension on the SL ligament?
Dart throwers motion
- Radial-extension to ulnar-flexion
What percentage of patients with a DISI progress to SLAC wrist?
[JAAOS 2015;23:691-703]
<5-10%
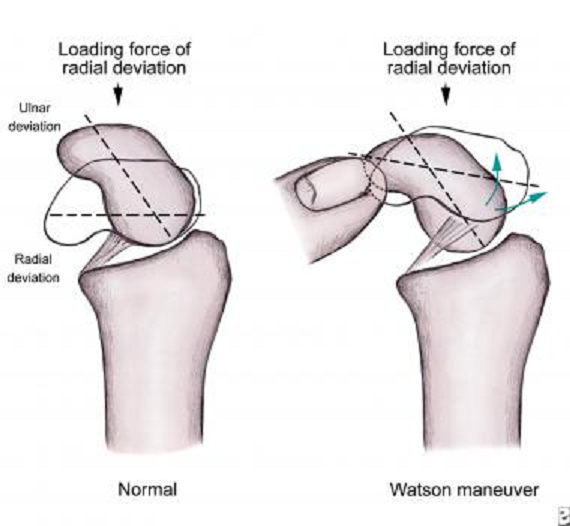
Describe the Watson Scaphoid Shift test?
[JAAOS 2015;23:691-703]
Examiner provides dorsally directed pressure on the scaphoid tubercle while ranging the wrist from a position of ulnar deviation with slight extension to radial deviation with slight flexion
- If SLIL is injured:
- Dorsal pressure subluxates the scaphoid onto the dorsal rim of the radius
- When pressure is released, a palpable clunk and reproduction of dorsal wrist pain occur as the scaphoid relocates into the radioscaphoid fossa.
What are the radiographic classifications of SL ligament injury?
[JAAOS 2015;23:691-703]
- Static instability
* SL instability evident on plain film - Dynamic instability
- SL instability evident on stress views
- Stress view = AP clenched fist with 30° ulnar deviation
- Predynamic instability
* SL injury evident on advanced imaging or arthroscopy
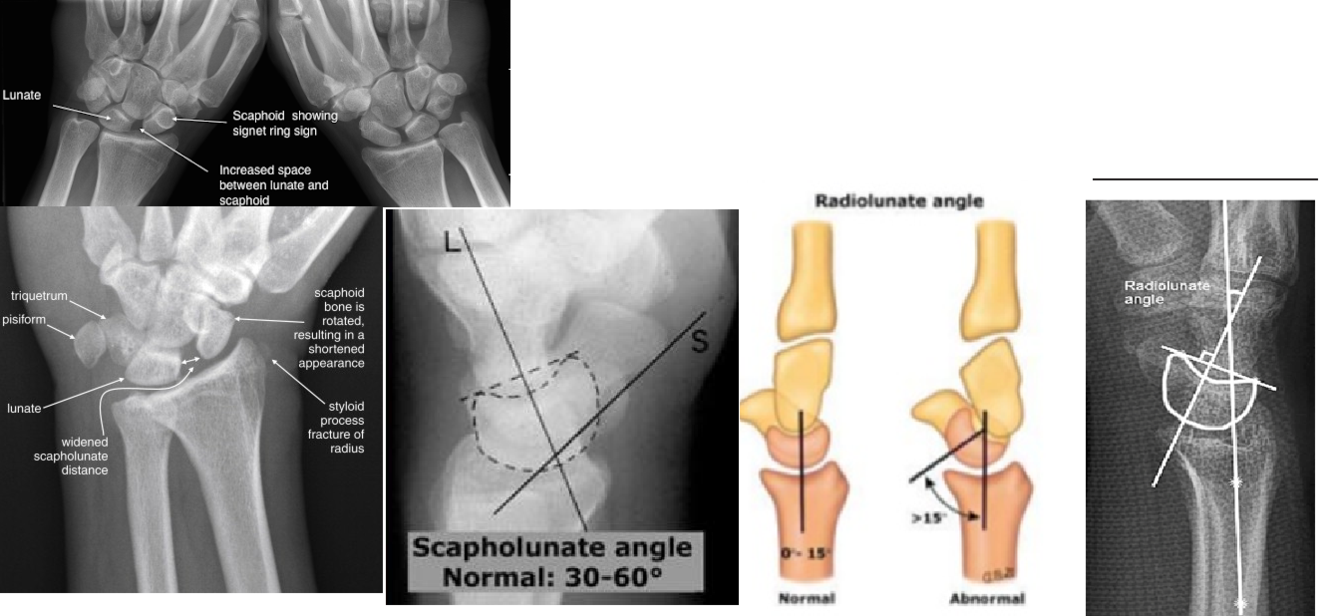
What are the radiographic features of a SL ligament injury?
[JAAOS 2015;23:691-703]
- Widened SL distance
- Cortical ring sign
- Shortening of the scaphoid
- Scapholunate angle >70° (normal = 30-60)
- Lunate extension
- DISI defined by radiolunate angle >15°
What arthroscopic portal is the SL ligament best visualized from?
[JAAOS 2015;23:691-703]
Visualized from the radiocarpal space through the 3-4 portal
- Probe in the 4-5 or 6R portal
What is the arthroscopic classification of SL ligament injury?
[JAAOS 2015;23:691-703]
Geissler Classification
- Stage I
- 1mm probe cannot enter SL space from midcarpal joint
- Stage II
- 1mm probe can enter SL space from midcarpal joint but not rotate 90°
- Stage III
- 1mm probe can enter SL space from midcarpal joint and rotate 90°
- Stage IV
- 2.7mm scope can drive through the SL space from the midcarpal and radiocarpal joint
What are the surgical options for managing SL ligament injury?
[JAAOS 2015;23:691-703]
- Primary repair
- Repaired with two horizontal mattress sutures through bone tunnel or suture anchor
- Protected with K-wire or screw augmentation
- +/- capsulodesis augmentation
- Indicated for acute tears
2. Arthroscopic debridement - Indicated for symptomatic partial tears
3. Reconstructive procedures - Indicated for high grade tears with no arthritis
- Blatt capsulodesis
- Capsular flap is attached to the distal scaphoid to prevent flexion
- Recommend using the DIC ligament
- ***Note – does not address the SL gap or lunate extension
- Capsular flap is attached to the distal scaphoid to prevent flexion
- Modified Brunelli procedure
- Portion of the FCR from the base of the 2nd metacarpal is passed through the distal scaphoid and attached to the dorsal lunate
- Ligament reconstruction
- Most common donor site is retinaculum of the third dorsal compartment of the wrist with bone blocks from the distal radius
- RASL
- ‘Reduction and association of the scaphoid and lunate’
- Herbert screw fixes the scaphoid and lunate to create a fibrous union (‘neoligament’)
- Salvage Procedures
- Indicated for high grade tears with arthritis
- Arthroscopic debridement
- Radial styloidectomy
- Wrist denervation
- PRC
- 4-corner fusion
- Limited carpal fusion
- Arthroplasty
- Total wrist fusion
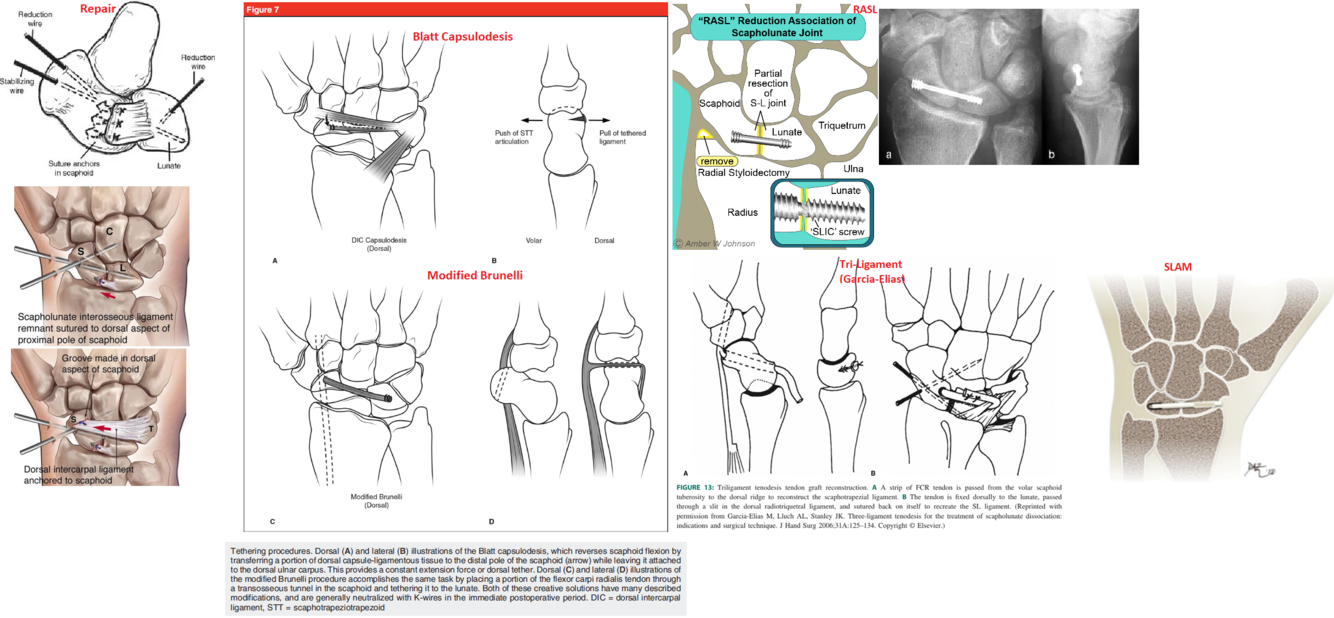
What is the technique for a Blatt capsulodesis?
- Original technique
- Utilized a strip of dorsal wrist capsule attached to the distal radius and inserted onto the distal pole of the scaphoid preventing scaphoid flexion
- Disadvantage
- Wrist flexion limited by ~20° due to crossing of the radiocarpal joint
- Modified DIC capsulodesis
* Detaches the proximal portion of the DIC from the triquetrum and after reduction of the scaphoid flexion it is attached to the lunate
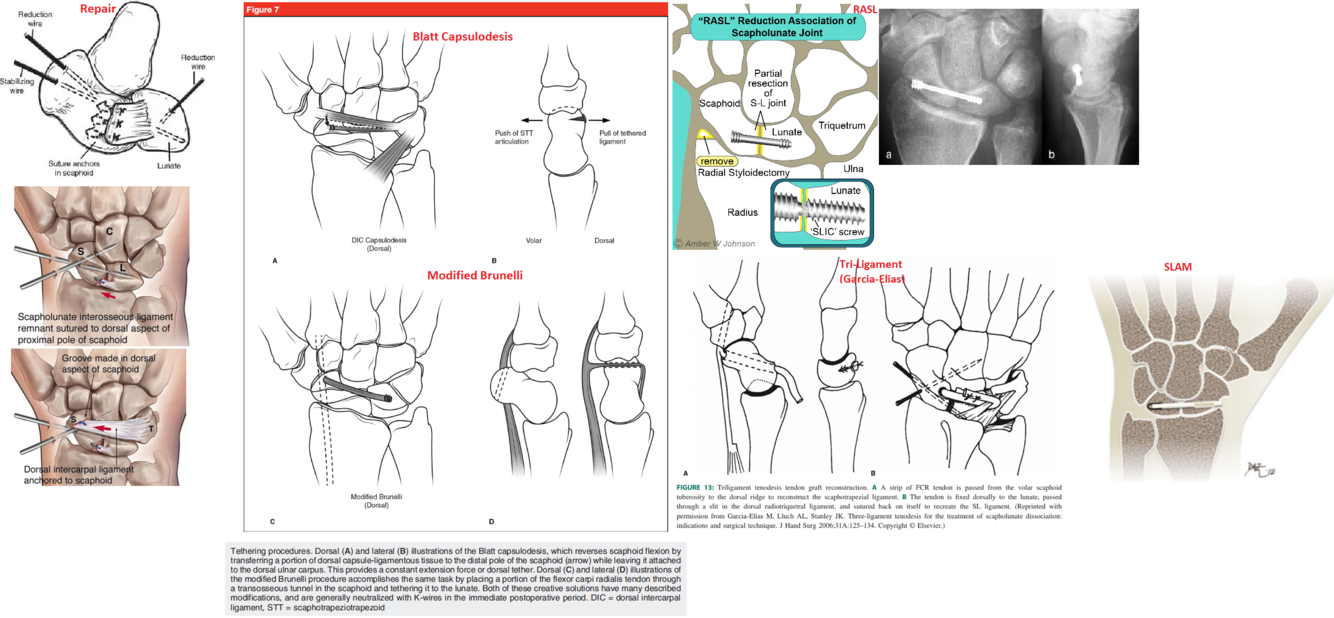
What is the technique for the Brunelli procedure?
- Dual volar and dorsal incisions
- A portion of the FCR is passed through the scaphoid tuberosity and sutured to the remnants of the SLIL on the dorsal aspect of the scaphoid.
* The remaining portion of the FCR slip is anchored to the dorsal ulnar corner of the distal radius
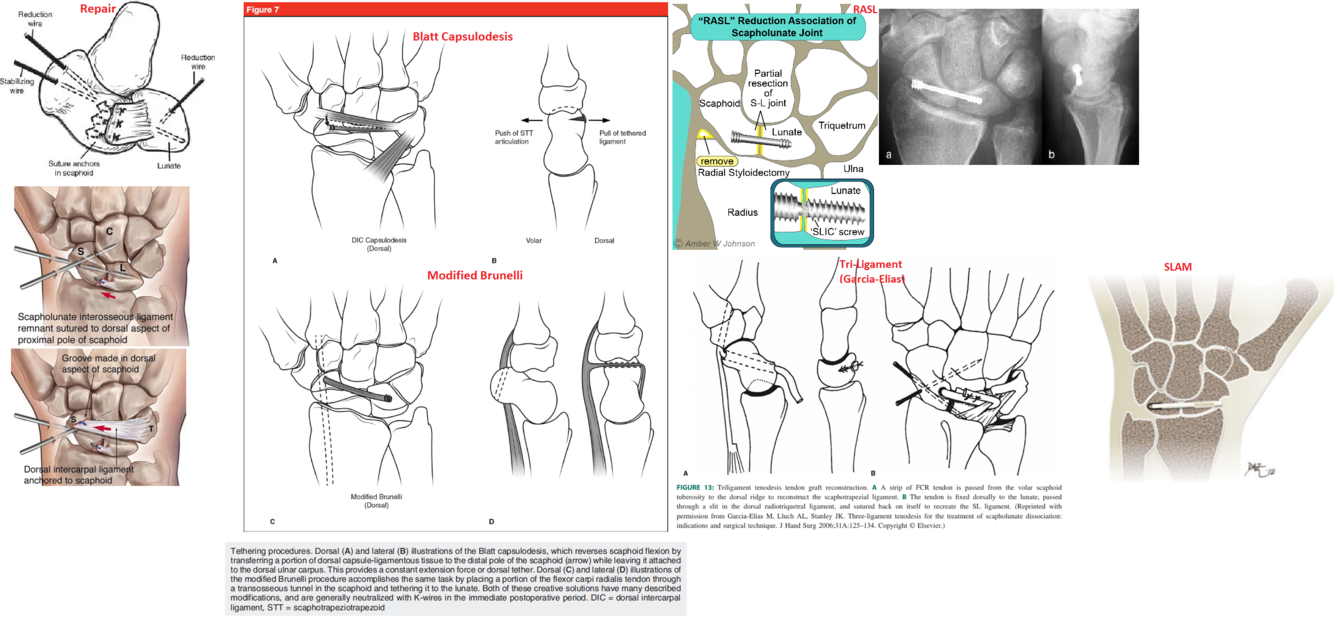
What is the technique for the modified Brunelli procedure?
Triligament tenodesis described by Garcia-Elias
- A strip of FCR tendon is passed from the volar scaphoid tuberosity to the dorsal ridge to reconstruct the scaphotrapezial ligament
- The tendon is fixed dorsally to the lunate, passed through a slit in the dorsal radiotriquetral ligament, and sutured back on itself to recreate the SL ligament.
What is the most common pattern of wrist arthritis?
SLAC (55%)
What is the pathomechanics of SLAC and SNAC wrist development?
- In the normal wrist:
- Scaphoid links the proximal and distal carpal rows
- Proximal row moves with the scaphoid
- Scaphoid has a tendency to assume a flexed posture
- Capitate longitudinal load on the lunate is eccentric causing the lunate and triquetrum to extend
- These forces are balanced as long as the link between the scaphoid and lunate are intact
2. With SL ligament disruption: - The scaphoid flexes and lunate/triquetrum extend independently
- Radiolunate joint remains congruent with lunate extension
- Radiolunate joint preserved
- Radioscaphoid joint becomes incongruent with scaphoid flexion
- Radioscaphoid degeneration progresses
- With scaphoid nonunion
- The distal scaphoid flexes
- The proximal scaphoid extends with the lunate and triquetrum
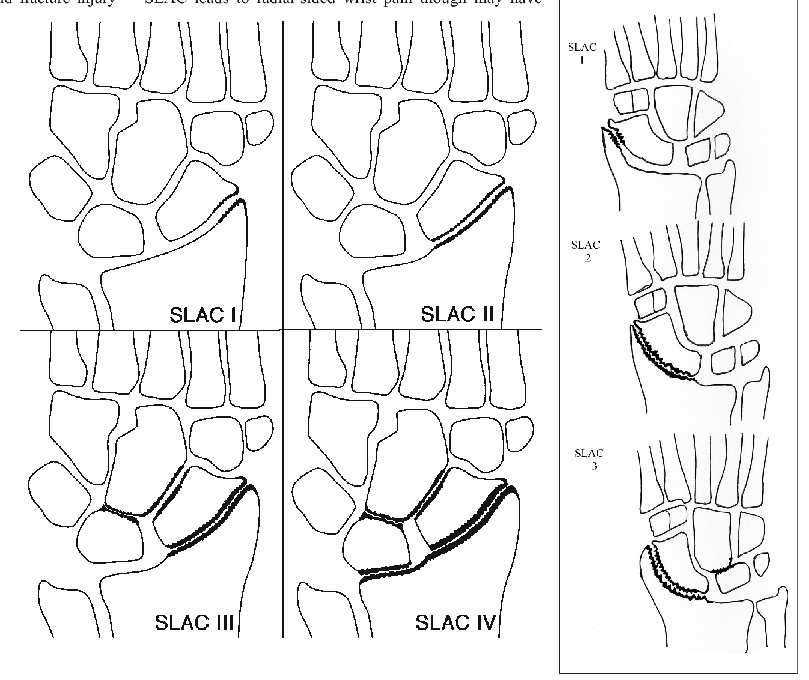
What are the radiographic stages of SLAC wrist?
Stage I - radial styloid
Stage II - radioscaphoid joint
Stage III - capitolunate joint
[Stage IV - pancarpal involvment (controversial)]
***Radiolunate typically spared
Initially, degeneration occurs between the radial styloid and radial side of scaphoid near the waist
- Degeneration progresses to the proximal pole involving the entire radioscaphoid joint
- With scaphoid flexion and loss of the link between the distal and proximal rows increase load occurs in the midcarpal joints (loss of buttress)
- Capitolunate degeneration develops with eventual migration of the capitate proximally between the scaphoid and lunate
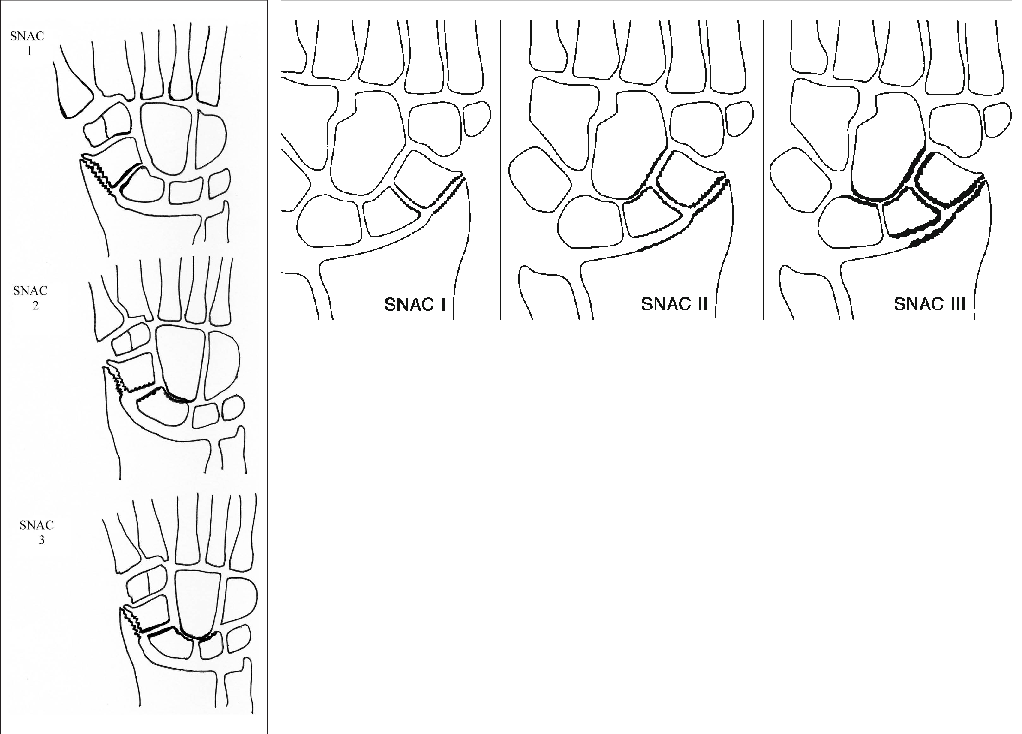
What are the radiographic stages of SNAC wrist?
Stage I - radial styloid
Stage II - proximal scaphocapitate joint
Stage III - capitolunate joint
Initially, degeneration occurs between the radial styloid and radial side of the distal scaphoid fragment
- Degeneration does not progress proximally in the radioscaphoid joint because the proximal scaphoid relationship with the lunate is maintained
- Degeneration progresses to the midcarpal joint starting with the proximal scaphocapitate joint then the capitolunate joint
What are the treatment options for SLAC and SNAC wrist?
Stage I
- Radial styloidectomy
- Distal pole excision (SNAC)
- Wrist denervation (AIN and PIN)
Stage II
- Proximal row carpectomy (PRC)
- Four corner fusion
Stage III
- Four corner fusion
- [PRC with capsular flap interposition]
(Stage IV – pancarpal)
- Total wrist fusion
- Total wrist arthroplasty
what are the advantages and disadvantages of PRC and 4 corner fusion
- PRC
- advantages - greater postop ROM (flexion, extension, total flexion/extension arc), lower complication rate
- others - earlier ROM no hardware
- 4 corner fusion
- advantages - greater radial deviation ROM, greater grip strength













































































































-
Plate/Screw/Nail Principles (updated)27
-
Trauma Principles (ex-fix/skeletal traction, nonunion, bone defect, HO, arthrodesis, nec fasc, comp sx, tendon transfer) updated83
-
Trauma - (DCO, FES, GSW, amp, morel-lav) updated23
-
Trauma - Upper Extremity205
-
Trauma - Pelvis/Acetabulum110
-
Trauma - Femur/Tibia174
-
Trauma - Foot and Ankle133
-
Paeds Trauma163
-
Paeds Non-Hip173
-
Paeds Hip51
-
Paeds CP23
-
Paeds Spine64
-
Knee Arthroplasty (updated)182
-
UKA updated11
-
Hip Arthroplasty (updated)115
-
Revision Hip/Knee Arthroplasty48
-
PJI updated23
-
Spine (Updated)236
-
Shoulder127
-
Elbow120
-
Hand and Wrist (Updated)255
-
Foot and Ankle169
-
Oncology89
-
Sports - Upper Extremity153
-
Sports - Lower Extremity313
-
Sports - Paeds14
-
Genetic Abnormalities13
-
Medical Conditions18
-
Research Study Summaries14
-
Approaches55
