Glomerular Disease Pathology Flashcards
What is glomerulonephritis?
Inflammation of the tinu filters in your kidney (glomeruli)
What is inflammation of the glomeruli called?
Glomerulonephritis
How does blood enter the glomerulus?
Via afferent arteriole
What happens once blood enters the glomerulus?
Some of it is filtered across glomerular membrane

When blood enters the glomerulus, what happens to albumin and porteins that are equal in size or larger?
They are not filtered and will stay in plasma
What are the cells called in the Bowman’s capsule that wrap around the capillaries of the glomerulus?
Podocytes
What are podocytes observed to have?
Interdigitating fingers or foot processes

What can be seen if you took a secrtion through a capillary loop?
Filter barrier, which is a membrane composed of endothelial cell cytoplasm, basal lamina and podocyte
What are the 3 parts of the filter barrier?
Endothelial cell cytoplasm
Basal lamina
Podocyte

What are mesangial cells?
‘Tree like’ group of cells which support capillaries

What happens to filtrate after glomerulus?
Goes into Bowman’s space, then into proximal tubule
After the glomerulus, what do blood cells, some fluid and albumin and larger proteins exit via?
Efferent arteriole

What are the different kinds of glomerulonephritis?
Inflammatory or non-inflammatory
Primary (only affects glomerulus) or secondary (other body parts affected such as SLE or Wegener’s)
What is primary glomerular disease?
Only affects glomerulus - idiopathic
What is secondary glomerular disease?
Kidney conditions with glomerular pathology in which an underlying cause can be established
- Affects other parts of the body
What are examples of diseases causing secondary glomerular disease?
Systemic lupus disease
Diabetes
Granulomatosis with polyangiitis (wegners)
drugs
What is the aetiology of glomerulonephritis?
Some are due to immunoglobulin deposition and some are diseases with no immunoglobulin deposition, such as diabetic glomerular disease
What are the 4 common presentations of glomerulonephritis?
- Haematuria (blood in urine)
- Heavy proteinuria (nephrotic syndrome)
- Slowly increasing proteinuria
- Acute renal failure
What is the medical term for blood in urine?
Haematuria
What is the medial term for excess proteins in the urine?
Proteinuria
What are different conditions that caue glomerulonephritis?
IgA glomerlonephritis
Membranous glomerulonephritis
Diabetic nephropathy
Crescentic glomerulonephritis
What does IgA glomerulonephritis often present with?
Often presents with discoloured urine, investigation would be dipstick urine which is positive for blood
What are the main causes of haematuria?
- Urinary tract infection
- Urinary tract stone
- Urinary tract tumour
- Glomerulonephritis
What are the main causes of IgA glomerulonephritis?
Idiopathic however is associated with:
- genes
- liver diseases
- coeliac disease
- infections
What investigations are done for IgA glomerulonephritis?
Dipstick urine
Urine culture
Ultrasound scan
If all normal, renal biopsy
If all typical investigations are normal for IgA glomerulonephritis, what investigation would be done?
check clotting factors then do Renal biopsy
What is immunofluorescence?
Method in biology that relies on the use of antibodies chemically labeled with fluorescent dyes to visualize molecules under a light microscope
What can be done with renal biopsy in IgA glomerulonephritis?
Only a biopsy can show the IgA deposits in the glomeruli.
The biopsy can also show how much kidney damage has already occurred.
Allows for management options to be discussed.
What is seen in a renal biopsy and immunofluorscence for IgA glomerulonephritis?
- Reveals immunoglobulin (of IgA type) and complement component of C3 in mesangial area of all glomeruli
What is the aetiology of IgA glomerulonephritis?
Aetiology of IgA glomerulonephritis is unknown:
- Excess antibody (IgA) sometimes present in serum, but this is also true of some people who do not have IgA glomerulonephritis
What is the pathogenesis of IgA glomerulonephritis?
IgA also does not get filtered into urine, it is “stuck” within the mesangium
This causes mesangium, not the filter membrane to become clogged with antibody – causing red blood cells to escape into urine:
- IgA irritates mesangial cells and causes them to proliferate and produce more matrix
What is the prognosis of IgA glomerulonephritis?
- Usually self-limiting, ie return to normal
- Small percentage go onto chronic renal failure (via continued deposition of matrix)
What is the typical presentation of membranous glomerulonephritis?
Could present with feeling unwell and swollen legs and protrinurea (albumin in urine)
What investigations are done for membranous glomerulonephritis?
- urine dipstick
- urine culture
- abdominal ultrasound
- Check clotting screen then do renal biopsy
What is seen in a dipstick of urine for membranous glomerulonephritis?
Proteinuria
What is seen in blood biochemistry for membranous glomerulonephritis?
Serum albumin low
What is the pathogenesis of membranous glomerulonephritis?
In membranous glomerulonephritis IgG is stuck in the membrane:
- IgG deposits itself between basal lamina and podocyte but cannot go further and is not filtered into urine
- IgG is too big to be filtered into urine, but activates complement (C3) which punches holes in filter
- This leaky filter now allows albumin to be filtered into urine, causing nephrotic syndrome
What does renal biopsy reveal for membranous glomerulonephritis?
Thickened glomerular basement membrane
Deposits of IgG
Basal lamina spikes (matrix which tries to surround the deposit)
What is deposited on the membrane in membranous glomerulonephritis?
IgG
What is the prognosis of membranous glomerulonephritis?
- 1/4 will get chronic renal failure within 10 years
What is the aetiology of membranous glomerulonephritis?
- Unknown but ca sometimes have underlying malignancy
- In many patients antigen is phospholipase A2 receptor
What investigations are done for diabetic nephropathy?
Dipstick urine
Clotting screen
Renal biopsy
What can be seen in the biopsy for diabetic nephropathy?
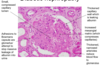
What is the pathogenesis of diabetic nephropathy?
glomerular sclerosis and fibrosis caused by the metabolic and hemodynamic changes of diabetes mellitus. It manifests as slowly progressive albuminuria with worsening hypertension and renal insufficiency.

What kind of lesion does diabetic nephropathy cause?
Diabetic nephropathy causes nodules of mesangial matrix to form, known as Kimmelsteil-Wilson lesion:
- Is gross excess of mesangial matrix forming nodules

What is the prognosis of diabetic nephropathy?
- Inevitable decline if established diabetic nephropathy ad if continued poor diabetic control
What is a sign of acute renal failure?
Rapidly rising creatinine
What are the typical investigations for renal disease?
Urine dipstick
urine culture
abdominal ultrasound
Clotting screen
Renal biopsy
What is seen in the biopsy for crescentic glomerulonephritis?
Early endothelial damage with fibrin deposition
Crush glomerular tuft
Cellular proliferation and influx of macrophages (is the crescent) around glomerular tuft, within Bowman’s space

What are some causes for the crescentic glomerulonephritis pattern of injury?
- Granulomatosis with polyangiitis (also known as Wegener’s granulomatosis)
- Form of vasculitis (inflammation in vessels) which affects vessels in kidneys, nose and lungs
- Microscopic polyarteritis (a disease very like Wegener)
- Antiglomerular basement membrane disease
- Many other forms of glomerulonephritis
What is granulomatosis with polyangitis also known as?
Wegener’s granulomatosis
What is Wegener’s granulomatotis?
- Form of vasculitis (inflammation in vessels) which affects vessels in kidneys, nose and lungs
What further tests can be done for Wegener’s?
- Serum test shows presence of anti-neutrophil cytoplasmic antibodies (ANCA)
- These are not deposited in the kidneys
- Antibodies directed against proteinase 3 and myeloperoxidase, 2 enzymes in primary granules of neutrophils
- Antibodies produce tissue damaged via interactions with primed neutrophils and endothelial cells
What do serum tests reveal in Wegener’s?
Presence of anti-neutrophil cytoplasmic antibodies (ANCA)
What does ANCA stand for?
Anti-neutrophil cytoplasmic antibodies
What is ACNA a form of?
Autoimmunity
What is the prognosis of Wegener’s?
- Fatal (mean survival time is 6 months) if left untreated
- Cyclophosphamide
- 75% complete remission
