Exam 1 Spring Flashcards
Inferior innominate shear
§side with the POSITIVE standing flexion test.
- ASIS on affected side is inferior
- PSIS on affected side is inferior
- Pubic rami on affected side may be inferior
Ischial tuberosity inferior



Seated & Standing Flexion Tests: sacrum & ileum
Sacrum-
- seated FT lower extremities = not influencing SIJ
- positive test indicates the side (lateralization) but not the specific dysfunction, of sacroiliac dysfunction.
Ilium-
- during the standing FT the lower extremities = influence SIJ
- positive test indicates an iliosacral SD, or excessively tight contra-lateral hamstrings.
Joints significant in gait

-Deep sulcus and post/inf
ILA are opposite so we have
an oblique axis
-The sacrum has rotated
towards the right; L5 rotated to
the left
Dx: R on R sacral torsion

Shuffling gait
typ in parkinson’s
pattern:
- small, flat-foot shuffle (less ground clearance)
- rigid, temor, pausing mvmts, shuffling with haste,
- diff: start, stop, turn
- trucal flex
1st noticable signs: non-rhyth pattern with random/poor timed arm swings
tx: L-dopa

cranial concept of pelvis
sacrum connects innominates –> occiput motion
alts affect either side: alters biomech model via dural attachement
Superior Innominate shear
§shear-named for the side with the POSITIVE standing flexion test.
- ASIS on affected side is superior
- PSIS on affected side is superior
- Pubic rami on affected side may be superior
- Ischial tuberosity superior

Ataxic gait
reeling, unsteady with wide base: tend to fall towards side of lesion
pattern:
- irreg steps
- lateral veering
- carefully watching ground
most prominent with sudden turns/stop/start
reasons:
- injury to cerebellum, SC, peripheral sensory NS
- inpair of joint position sense: afferent fibers disruption in peripheral N/posterior roots/posteiror columns of SC

Spondylolisthesis
anterior slippage of vert: usu @ L5 on S1

Low Back Pain Expanded Differential Dx (10)
PPP A A COMIC
Prostatitis
Paget’s disease
PID
AAA
Abscess
Ca lesions
Ovarian cysts/CA; endometriosis
Multiple myeloma
Infection
Compression fracture
pubic shear
subjective complaints?
caliper: gapping
subjective:
- UTI symptoms: burning, freq, fullness, weak stream, dysuria, dysparunia (painful sex)
Muscular Action during STANCE Phase

most important part of gait
flex of stance knee
if knee locked up = E expend up 50%
- another detm lost = 300% lost
Sacral/Innominate Motions during Gait
- Weight shift to the left
- Posterior rotation of innominate
- Rotation of whole pelvis to the left
- L/L sacral torsion

Innominate/Iliosacral Rock/ Compression Test

Lower Extremity Joints during Gait: Ankle
body wt = just medial of center: eversion –> inversion
Forward Sacral Torsions with Gait

Left stance leg =
Left on Left torsion
Right stance leg =
Right on Right torsion
Traumatic Sacral SD
slip/fall on butt
MVC –> F from “braking” foot –> leg –> pelvis
Anterior SIJ
synovial
different orientation than posterior/lig aspect

herniated disc
type 2 F SD –> flat lordosis –> shearing stress
rad pain –> butt
- init disinterpred as SI pain/dysfx
neuro exam important for distinguishing SI pain from disc protrusion
Forward Sacral Somatic Dysfunctions on Oblique Axis
- We have 4 possibilities for forward sacral somatic dysfunctions:
- Left on Left sacral torsion
- Left on left sacral rotation
- Right on Right sacral torsion
- Right on Right sacral rotation
what does the external oblique form distally?
inguinal lig as it txverses ASIS –> pubic tubercle


Sacral Torsion Rules
- Rule #1: When L5 is sidebent, a sacral oblique axis is engaged on the SAME side as the sidebending.
- Rule #2: When L5 is rotated, the sacrum rotates the opposite way on an oblique axis.
- Rule #3: The seated flexion test is found on the opposite side of the oblique axis.
respir-circ model of pelvis
pelvic diaphragm & bone –> interstitial homeostasis
M affecting ilial/pubic motion
RAGS
Rectus femoris
Adductors
Gracilis
Sartorius
hypertonia = pubic, ant/med knee pain
posterior SI lig
referred pain to hip and groin
connects PSIS –> S3/S4, erector spinae, thoracic/lumbar fascia
6 Determinants of Gait:
4 + 5
combined actions of the foot, ankle and knee of the stance leg
smooth pathway:
- heel strike: ankle form dorsi –> plantar flex (knee @ fulcrum)
- heel lift: metatarsal P (plantar flex) lifts COG, counteracted by knee flex
Forward Sacral Somatic Dysfunctions on Oblique Axis
- Left rotation of the sacral base on a left oblique axis with L5 rotated right = Left on Left forward sacral torsion
- Right rotation of the sacral base on a right oblique axis with L5 rotated left = Right on Right forward sacral torsion
- Naming Rule: we name the direction of sacral rotation 1st followed by the oblique axis. So a left on left sacral torsion means the sacrum has rotated left on a left oblique axis.
intraspinal dura attaches …
posterior longitudinal ligament of S2:
integrates cranial base with sacrum
subjective complaints of Inferior Innominate Shear
clincal?
pelvic pain with tiss-tex changes @: ipsilat SI jt & pubis
rare –> usu corrected with ambulation
clinical: bungee jumping
Muscular Action during STANCE Phase
before heel strike: dorsiflex contract concentrically
after hell strike –> onto foot flat: dorsiflexors contract eccentrically

possible ways to distinguish functional vs. structural leg length issue?
functional:
- ant-innominate rotation with ipsi med-malleolus lower
structural:
- ant-innominate rotation with ipsi med-malleolus higher
- ant-innominate rotation without change in leg length
- innominate resolved but now medial malleolus ipsi higher after OMT
Normal sacral motion during ambulation only involves
•anterior motion of the sacrum around these oblique axes
does not move posterior during normal walking cycle
waddling gait
roll side to side: penguin walk - pelvic rotation/tilt on swing side = increased
causes:
- muscular dystrophy
- weak hips
- exaggerated lordosis
- pot-bellied posture

subjective complaints of superior innominate shear
clincal scenario?
pelvic pain with tenderness @:
- ipsi SI jt
- QL
- pubic rami/symphysis
Clinical scenario; patient misjudges last step of stairs or curb, landing hard on the ipsilateral foot, creating a superior shear.

-Deep sulcus and post/inf
ILA are opposite so we have
an oblique axis
-The sacrum has rotated
towards the right; L5 rotated to
the left
Dx: R on L sacral torsion
Left Unilateral Sacral Flexion OMT
pt on stomach
- abduct/interal rotation lower extremity –> post sacral base
- respir assistance –> engage barrier with hand

•The seated flexion test will be ________ on the ______side of the deep sulcus in a ________ sacral dysfunction on an oblique axis, _______ the axis
positive
same
forward
opposite
Antalgic Gait
pain

Left Unilateral Sacral Extension
pt on stomach, tv stance
- abduct/internal-rot LE –> sacral base anterior
- respir assistance: engage barrier with hand

How to Differentiate Forward vs. Backward Sacral Dysfx
- Seated Flexion Test
- L5 mechanics: type I for forward; type 2 for backward
- Spring Test
- POSITIVE with Backward Sacral dysfx; Will not spring, non-compliant to posterior to anterior spring if sacral base is posterior.
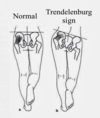
Trendelenburg Test
Superior gluteal nerve palsy
- Fracture neck of femur
- Dislocation of hip
- Perthe’s disease: avascular necrosis of head of femur, late stages of TB hip.
Posterior Innominate Rotations
named for the side with the POSITIVE standing flexion test
- PSIS on affected side is inferior
- ASIS on affected side is superior
- Pubic tubercle superior on affected side
- Ischial tuberosity inferior on affected side
- Motion about an inferior transverse axis

if the sacrum and L5 are rotated in the same direction ….
sacral rotation dysfx
tx:
- MET for sacral torsion
- L5
Pubic motion
Caliper: flex/extend
Torsional: swing-tilt
Supero-inferior: one legged wt-bearing
fib-cartilaginous jt
M forces = rotational about tx axis

ischiorectal fossa
•potential space between the inferior pelvic diaphragm and the urogenital diaphragm.

what do we know?
-Deep sulcus and post/inf
ILA are opposite so we have
an oblique axis
-The sacrum has rotated
towards the left; L5 rotated to
the left
Dx: L on L sacral rotation

Backward Sacral Rotations and Torsions
•Seated flexion test +
- •contralateral to deep sulcus and oblique axis
•THE SPRING TEST IS POSITIVE !!!
- oblique axis through the deep sulcus & post/inf ILA
•Sacral sulcus is shallow on dysfunctional side
- •By convention we consider and label the deep sulcus
- Posterior and/or inferior ILA
- L5 follows NON-neutral mechanics
Coccygodynia
pain in coccyx usu due to trauma
- also: infection, disloc, fx
pain = worse: sit/pooping strain/sex
- can be associated with pelvic diaphragm dysfx
Left on Left Sacral Torsion
neutral sacral mechanics (type 1)
- sit up, sidebend L –> L obliq axis
monitor:
- right index finger = anterior
- left thumb = post-/inferiorly.

•Sacralization of L5
L5 fused with sacrum

subjective complaints of anterior innominate
ipsilat hamstrin tightess (stretch)
sciatica (piriformis)
Unilateral Sacral Extension

Alternate Psoas Evaluation
pt prone
grab thigh above knee & extend hip: compare bilat
can get “end feel” of motion –> asses for type 2 SD @ L1/L2
Transverse Axes of the Sacrum
Superior Transverse Axis
“Respiratory or cranial” axis; associated with the attachment of the dura at S2
- inhale = base post, exhal = base ant
Middle Transverse Axis
“Postural” axis for flexion/extension spinal motions
- lumb-ext = base ant, lumb-flex = base post
Inferior Transverse Axis
Anterior/posterior rotation of the innominates on the sacrum around S3 segment.
pelvic girdle pelvic splanchnics
arise off ventral rami S2-S4
PNS to L colon & inferior mesenteric plexus
- mixes with visceral afferent and SNS
PNS visc-som refelx –> subQ swelling in sacral region
if doesn’t improve with tx –> look for imbalance or visceral origin
Spondylolysis
stress fx pars interarticularis: collar on scotty dog
common in adole atheles, esp gym with hyperext

Forward Sacral Rotations
around an Oblique Axis with Gait
- Left rotation of the sacral base around the left oblique axis occurs during the swing phase of the right leg.
- Right rotation of the sacral base around a right axis occurs during the swing phase of the left leg.
- If a normal, forward sacral rotation gets “stuck” in that position, it becomes a somatic dysfunction.
Most somatic dysfunctions in the sacrum involve forward torsions about an oblique axis.
Pubic Somatic Dysfunction
isolated = rare: usually assoc with innominate SD
respond well to ME: adductor M
consider anterior L5 tender pt (anterior rami) – counterstrain
DDx of pelvic congestion
- pelvic floor muscles vs. adductors vs visceral
- OB pt secondary to Relaxin.
Dysuria
“Failed Low Back Syndrome”
“last resort” for LBP

Scissors gait
legs add, cross alt in front of other
spastic lower limbs and hip jt add M
compensation motions of trunk and upper extremeties
causes:
- bilat UMN lesions
- cerebral palsy
- adv cerv spondylosis
- MS

Hemiplegic gait
due to: cva, SC injury
presentation:
- affected leg = stiff with less flex of hip/knee
- leg circumducted, body leans away
- shoe drag
- arm = fixed: elbow flexed, hand pronated, fist formed with thumb tucked in

Nutation
“nodding”
sacral base anterior –> sacral flexsion (biomech model)
stopped by sacrotuberous lig

Transverse Sacral Axes
- Superior Axis
- Respiratory
- Cranial-sacral
- Middle Axis
* Postural or Sacroiliac - Inferior Axis
* Iliosacral (Innominate rotation on sacrum)

High Steppage Gait
1st pattern
- toe touches first: paralysis pretib/fib M –> slapping noise with foot after
- leg raised high: abnorm knee/hip flex
2nd pattern:
- heel touches first: loss of position –> stomp
- bilat: ataxia, side-to-side reeling
- romberg’s sign - dysfx afferent of peripheral N/posterior roots

Musculoskeletal Gait Patterns
Gluteus medius lurch
Psoas gait
glut max/extensor lurch
Gluteus medius lurch - waddle side to side
Psoas gait - leans over
glut max/extensor lurch - leans backwards

Standing
- Width of the base (heel to heel) = 2-4”
- Feet - slight lateral rotation
- Only a few muscles usually active
–Erector Spinae
–Triceps surae
–Iliopsoas
- Forward sway
- Lateral sway

6 Determinants of Gait –
6
Minimizing lateral displacement of the Center of Gravity (COG)
stable gait = shift of COG to wt-bearing leg
add of hip & tib-fem angle = reduces lateral displace for balance

pelvis lig: true and accessory
true:
- Anterior sacroilliac ligaments
- Interosseous sacroiliac ligaments
- Posterior sacroiliac ligaments
accessory:
- Sacrotuberous
- Sacrospinous
- Iliolumbar

Oblique Axes of the Sacrum
named for superior pole of sacrum they pass thru
gait
- left stance leg/right swing: L oblique axis –> sacral base moves anterior on R, ILA moves post/inf on L

sacral development
5 segments:
lateral –> body: 2 years
sacral seg sep by IV disc until 25-30

Backwards Sacral Dysfunction
- In this situation, the sacral base has moved posteriorly up the short arm of the SIJ o the side of the oblique axis.
- The anterior part of the sacrum is facing left, although it’s from the left part of the sacral base moving posteriorly.
- This is associated with a Type 2 L5 somatic dysfunction, and is commonly caused by a flexion and sidebending type of injury to the L/S junction that drives the sacral base posteriorly.

Counternutation
sacral base moves posteriorly
Motion is checked by posterior SI ligaments

Q – angle
angle b/w femur and tibia
increased in women: wider hips

•Dx = L on R sacral torsion
ME:
- L5 rot L, lower leg extended = sacral base anterior
- pt contract L QL –> R QL recip-inhib


Thomas Test- psoas spasm
increased distance b/w knee and table = positive
Swing Phase – Mid-swing
mostly momentum
knee extension added

axes of sacrum

- Superior transverse axis
- Middle transverse axis
- Inferior transverse axis
- Left oblique axis
- Right oblique axis
Sacro-ilitis (Ankylosing Spondylitis)
inflam SIJ: bilat
negative for rheumatoid factor
genetic: HLA-B27
males: disease moves up spine, female = begin anywhere without pattern
bamboo spine (fusion) as disease progresses - the outer fibers of annulous fibrosis ossify and the vertebra become more square

What do we know?

What do we know?
-Deep sulcus and post/inf
ILA are opposite so we have
an oblique axis
-The sacrum has rotated
towards the left; L5 to the right
-Torsion
Dx: L on L sacral torsion
Unilateral Sacral Flexion
seated flexion test is positive on the same side which is “stuck” in flexion

what do we know?

-Deep sulcus and post/inf
ILA are opposite so we have
an oblique axis
-The sacrum has rotated
towards the left; L5 to the right
-Torsion
Dx: L on R sacral torsion
L5 FRrSr because backwards dysfx
follows type 2 mechanics
Introduction to Gait

- Average step length = 15”
- Cadence of 90-120 steps per minute

Psoas Syndrome
type 2 SD F L1/L2
- ipsi lumbar SB, contralat rot
sacral SD = same side as SB
pelvic shift, piriformis, sciatic irritation = opp of spasm
chronic: fwd sacral torsion –> engage oliq axis with lumbar SB
acute: L1/L2 F, L5 E (type 2) –> bwd sacral torsion

Muscular Action during SWING Phase

Floor contact as foot progresses: gait

Anterior Innominate Rotation
named for side with POSITIVE standing flex test
- ASIS on affected side is Inferior
- PSIS on affected side is Superior
- Pubic tubercle inferior on affected side
- Ischial tuberosity superior
- Motion about an inferior transverse axis

Innominate Flares
flare = ASIS more medial on one side vs other
measure from xyphoid/umbilicus –> each ASIS
named for side of postiive standing flex test

Spring Test
spring lumbo-sac jxn with hell of hand
ease = NEGATIVE
resistance = POSITIVE - bwkwards sacral dyfx
