Describe how the endometrium is affected by the menstrual cycle
Endometrial growth in the functional layer is stimulated during the follicular phase of the menstrual cycle by estrogen (via LH) and then by porgesterone from the corpus luteum in the luteal phase of the menstrual cycle. If not fertilization occurs, the functional layer loses its stimulation from the CL and is sloguhed off during menses. Note that the basal layer of the endometrium remains in tact during menses
Describe the layers of the uterus as seen below
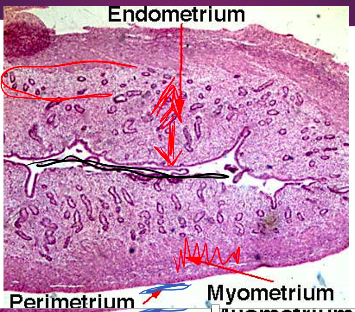
The body of the uterus is composed of three layers, the inner most endometrium (which is sloughed during menses), the muscular myometrium, and the outer perimetrium. Circled in this picture is the basal layer of the endometrium
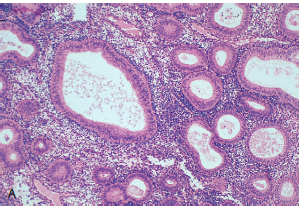
What does the endometrium look like during the proliferative phase of the menstrual cycle
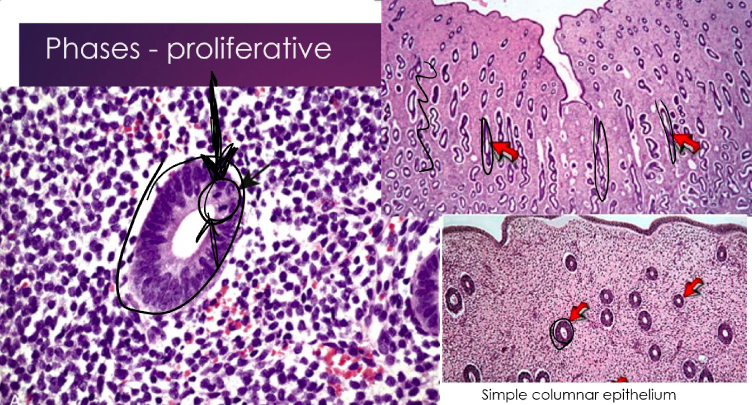
The glands are round, proliferative, and contain mitotic figures (not curly)
What does the endometrium look like during the secretory phase of menstruation?
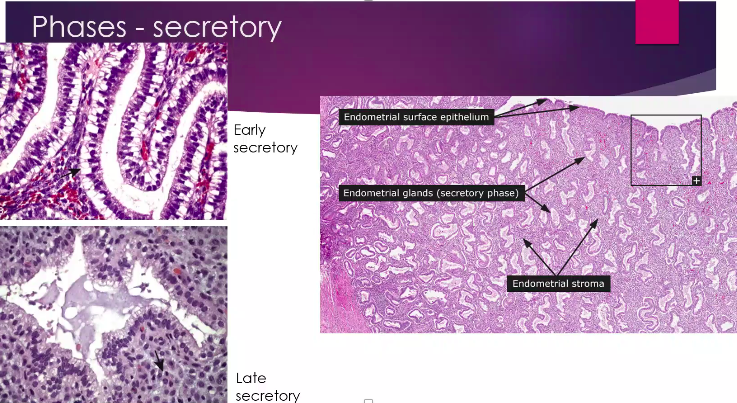
In the early phase, secretions inside the glands start to be seen and they become corkscrew shaped and sub-nuclei vacoules that eventually secrete into the lumen of the glands
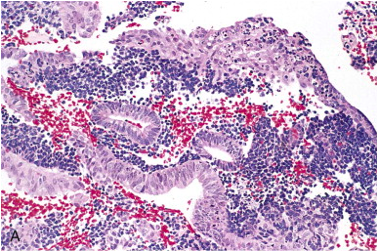
What does the endometrium look like during the menses phase of menstruation?
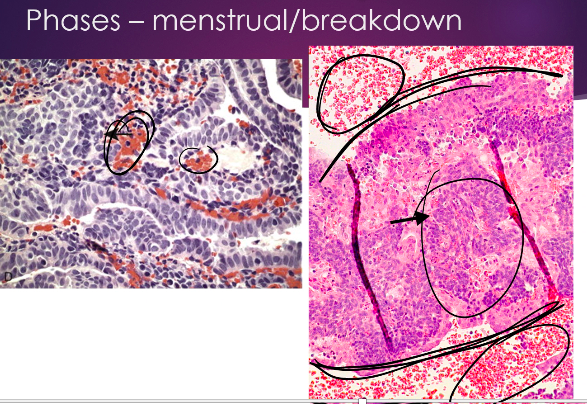
Tissue begins to almost ball up to be sloughed and hemorrhage can be seen
What are the common causes of dysfunctional uterine bleeding (bleeding from the uterus in the absence of an organic uterine lesion) in pre-pubertal children?
precocious puberty
What are the common causes of dysfunctional uterine bleeding in adolescence?
Anovulatory cycle, coag disorders
What are the common causes of dysfunctional uterine bleeding in reproductive age women?
complications of pregnancy (abortion, ectopic preg)
Anatomic lesiosn (leiomyoma, endometrial hyperplasia, carcinoma)
Anovulatory cycle
Ovulatory dysfunctional bleeding (e.g. inadequate luteal phase)
What are the common causes of dysfunctional uterine bleeding in peri-menopausal women?
anovulatory cycle
Anatomic tumors/lesions
Why would an anovulatory cycle be associated with bleeding?
Failure to ovulate leads to unopposed estrogenic stimulation of the endometrium with low progesterone which causes it to overproliferate and dilate and eventually the top layer breaks down and sheds. The endometrial glands may develop cystic changes and appear disorderly, while the endometrial stroma may be scarce (b/c it requires progesterone to grow)
Biopsy will read as a “disordered proliferative pattern with shedding’
Anovulatory cycles result from subtle hormonal imbalances and are most common when?
at menarche and in the perimenopausal period.
Less commonly, anovulation is the result of:
- Endocrine disorders , such as thyroid disease, adrenal disease, or pituitary tumors
- Ovarian lesions , such as a functioning ovarian tumor (granulosa cell tumors) or polycystic ovaries
- Generalized metabolic disturbances , such as obesity, malnutrition, or other chronic systemic diseases
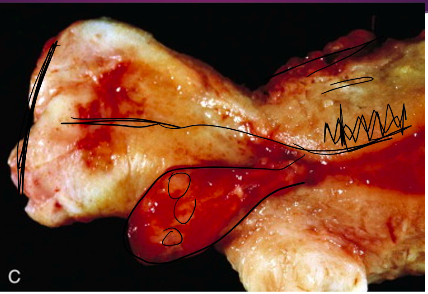
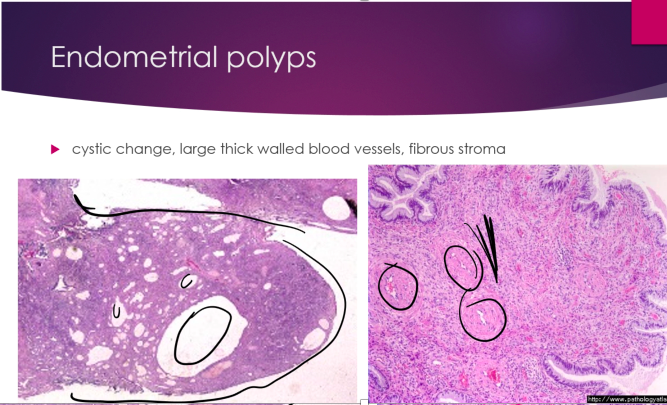
What is this?
Endometrial polyps are localized overgrowth of endometrial glands and stroma that present as a pedunculated mass typically as a result of unopposed estrogen. These typically dont turn malignant
Patients taking ______ are more likely to get endometrial polyps
tamoxifen (because tamoxifen has weak pro-estrogenic effects in the endometrium.). Hormone replacement and obesity can also increase the risk
T or F. Most endometrial polyps are unresponsive to progesterone
T. A few are hyperfunctional
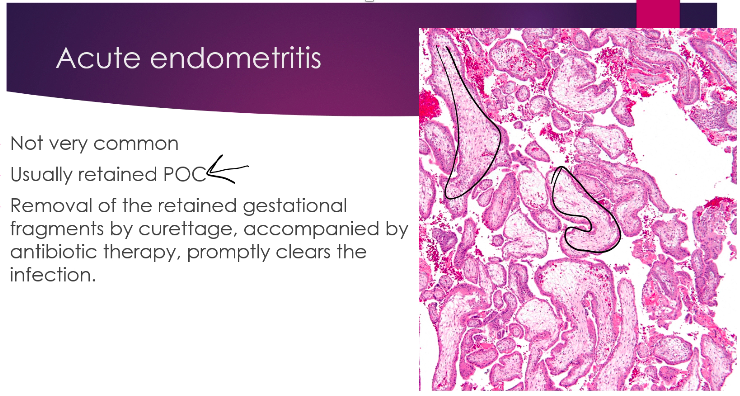
POC= product of conception (below- chorionic villi)
Look for plasma cells!!
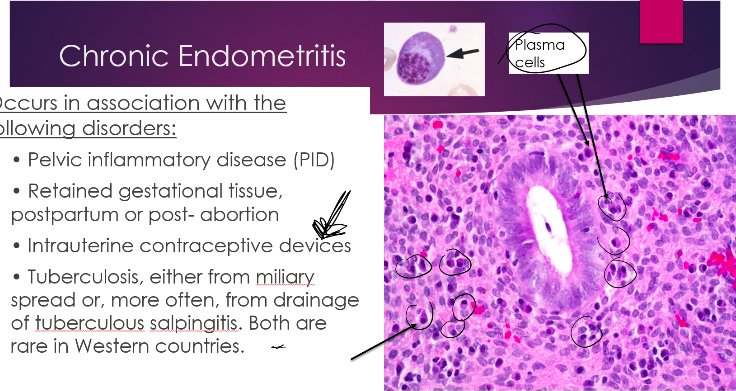
Infection with an IUD, think actinomyces
What is Endometriosis?
the presence of endometrial glands and stroma outside the endomyometrium. It occurs in as many as 10% of women in their reproductive yrs and nearly 50% of women with infertility
Where is endometriosis most commonly seen?
Most often pelvic structures (ovaries, pouch of Douglas, uterine ligaments) and less frequently distant areas of the periotoneal cavity and rarely even lungs, heart, and bone.
What causes endometriosis?
Is the displaced endometrial tissue in endometriosis normal or abnormal?
Abnormal in the sence that it exhibits increased levels of inflammatory mediators, particularly prostalandin E2, and increased estrogen production due to higher aromatase activity. These factors enhance this tissue’s ability to survive outside the uterus and can explain the beneficial effects of COX-2 inhibitors and aromatase inhibitors in tx.
When is adenomyosis?
the growth of the basal layer of the endometrium down into the myometrium between muscle bundles that commonly causes the myometrium to hypertrophy.
How mihgt adenomyosis present?
May produce menorrhagia, dysmenorrhea, and pelvic pain before the onset of menses












-
Female Anatomy Review48
-
Genetics of Sex Determination24
-
Male Anatomy Review10
-
Costanzo Ch. 1060
-
Female Hormones46
-
Male Hormones31
-
Female Puberty51
-
The Menstrual Cycle46
-
Costanzo Ch. 10 (2)20
-
Breast Pathology Pre-Study98
-
Cervix Pathology Pre-Study71
-
Male Puberty31
-
Disorders of Sexual Differentiation56
-
Tx of Breast and Endometrial Cancer58
-
Tx of Ovarian and Bladder Cancer22
-
Ovarian Pathology49
-
Tx of BPH30
-
Tx of Testicular Cancer23
-
Tx of Prostate Cancer32
-
Sperm Storage, Transport, and Male Sexual Dysfunction23
-
Endometrium Pathology54
-
Male Pathology81
-
Syphilis17
-
Trichomonas5
-
Mullerian Duct Abnormalities17
-
Inhibin and Actvin9
-
Diagnosing Disorders of sex hormones4
-
Pathoma Female67
