Connective Tissue Diseases Flashcards
(35 cards)
2 groups of connective tissue diseases
autoimmune diseases (target tissues themselves)
vasculitic diseases (vessels are targets)
autoimmune connective tissue diseases
- Multisystem vasculitic inflammatory diseases:
- Systemic lupus erythematosis (SLE)
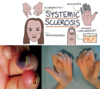
- Systemic sclerosis (Scleroderma)
- Sjogrens syndrome (SS)
- Undifferentiated connective tissue disease (UCTD)
- Have associated blood autoantibodies
- DO NOT cause the disease – are found in ‘normal’ people
- Pattern varies from disease to disease
Complement activation causes tissue damage
examples of autoimmune connective tissue diseases
Systemic lupus erythematosis (SLE)
Systemic sclerosis (Scleroderma)
Sjogrens syndrome (SS)
Undifferentiated connective tissue disease (UCTD)
features of autoimmune multisytem vasculitic diseases
- Have associated blood autoantibodies
- DO NOT cause the disease – are found in ‘normal’ people
- Pattern varies from disease to disease
- Complement activation causes tissue damage
vasculitis connective tissue diseases
3 categories
- Large vessel Disease
- Giant cell (temporal) arteritis
- Medium Vessel Disease
- Polyarteritis nodosa
- Kawasaki disease
- Small vessel Disease
- Wegener’s Granulomatosis
large vessel disease
giant cell (temporal) arteries
- Polymyalgia Rheumatica
medium vessel disease
polyarteritis nodosa
Kawasaki disease
small vessel disease
Wegner’s Granulomatosis
general management of connective tissue disease
- Dependant on disease activity
- Immune suppression – no cure as cause unclear
- Analgesic NSAIDs (joint/muscle symptoms)
- Immune modulating treatment
- Hydroxychloroquine
- Methotrexate
- Azathioprine
- Mycophenolate
- Biologic Medication – Cytokine inhibitors and lymphocyte depleting drugs
- Systemic steroids - prednisolone
immune connective tissue diseases are
interlinked
features overlap
pt presentation unique
Antibodies in Autoimmune diseases
- Anti-nuclear antibody (ANA)
- Anti-Ro antibody (Ro)
- Anti-La antibody (La)
overlap
- Anti-Scl-70 antibody
- Anti-Centromere antibody
- Anti-Neutrophil Cytoplasmic Antibody (ANCA)
last three sclerodoma

dicoid lupus
Tissue changes without blood autoantibodies called ‘Discoid Lupus’
- Seen in the skin and the mouth – looks similar to lichen planus
systemic lupus erythematosis
blood antibody changes
- Circulating immune complexes
- ANA, dsDNA & Ro antibodies
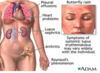
Multi-system
- joints, skin, kidney, muscles, blood
- CVS, RS & CNS
- Renal invlovement previously major cause
- Enhanced cardiovascular risk
12-64/100,000 population
Twins 20-50% concordance
- Siblings same as non-relatives 5%
females of child bearing age
photosensitivity common
- Butterfly zygomatic rash
- Generally avoid sun
systems affected in SLE
joints, skin, kidney, muscles, blood
CVS, RS & CNS
Renal invlovement previously major cause
Enhanced cardiovascular risk

circulating immune complexes in SLE
ANA, dsDNA and Ro antibodies

prevalance of SLE
- 12-64/100,000 population
- Twins 20-50% concordance
- Siblings same as non-relatives 5%
- females of child bearing age
photosensitive - avoid sun

dental aspects of SLE (7)
- Chronic anaemia
- oral ulceration
- GA risk
- Bleeding tendency
- Thrombocytopenia – bleeding tendency on extraction
- renal disease
- impaired drug metabolism
- drug reactions – photosensitivity
- steroid & immunosuppresive therapy
- Possible increased malignancy risk
- lichenoid oral reactions
- oral pigmentation from hydroxychloroquine use
lupus anticoagulant
Marker found in the blood of some patients with Lupus
- anticoagulates blood in a test tube but NOT in a patient
Indicates a ‘subtype’ of lupus patient
- These patients termed “antiphospholipid antibody syndrome”
- Primary Form
- No other associated disease
- Secondary Form
- Found in some patients with chronic inflammatory conditions e.g. SLE
- Primary Form
Antibodies
- Antiphospholipid (aPL)
- Anticardiolipin (aCL)
Can be primary – no other diseases associated with the antiphopholipid syndrome or secondary – lupus, sjörgen’s
Antiphospholipid Antibody Syndrome (APS)
- Characterised by recurrent Thrombosis
- DVT with pulmonary embolism
- Venous & arterial thrombosis
- Patients anticoagulated
- commonly on warfarin
- Do not stop anticoagulant – need physician advice

Sjögren’s syndrome
- Inflammatory disease ASSOCIATED with circulating autoantibodies
- ANA, Ro and La
- Mainly associated with dry eyes and dry mouth
- Multisystem in some
- Major involvement in Salivary glands
- Leads to Xerostomia and oral disease

3 main groups of sjögren’s
- Sicca Syndrome
- Dry eyes or Dry mouth
- Primary Sjögren’s
- Not associated with any other disease
- Secondary Sjögren’s
- Associated with another Connective Tissue disease – Rheumatoid Arthiritis, SLE, etc.
sjörgen’s syndrome diagnostic criteria
No one test that ‘proves’ Sjögren’s syndrome
Some signs/symptoms more important than others
- Dry eyes/mouth
- Subjective or objective
- Lacrimal and salivary glands changes can take 30 years to show clinically due to residual capacity– need histological exam to test properly
- Subjective or objective
- Autoantibody findings
- Imaging findings
- Histopathology findings
Positive criteria for diagnosis often a clinical judgement
Sicca syndrome sjögren’s
dry eyes or dry mouth
primary sjögren’s
not associated with any other disease
secondary sjögren’s
associated with another connective tissue disease - RA, SLE etc