CM: Bowel Mvt Changes Flashcards
In a FDR w/ colon cancer, what factor can help assess risk?
FDR’s age at dx, if >60 y/o, more likely sporadic than genetic; would not portend higher risk for patient
With recent change in bowl habits, what would be the next step to diagnose cause of diarrhea?
Colonoscopy
What would argue vs. a trial Tx for possible Irritable Bowel Syndrome?
Red flags such as weight loss, nocturnal bowel movements, etc- these would point to a more pathologic process rather than functional
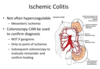
Assess the status of this colon on colonscopy

Normal w/ pale mucosa, uniformity in appearance and normal vasculature
With a normal appearing colonscopy, what would be the next step to assess patient’s diarrhea?
Random biopsies of normal appearing colon
Despite colon’s normal appearance on colonoscopy, what might a biopsy like this one reveal?

Lymphocytic Colitis, a type of microscopic colitis

Aside from Lymphocytic Colitis, what is another type of microscopic colitis?
Collagenous Colitis

What histologic features do Lymphocytic Colitis and Collagenous Colitis share? What is their distinction?
Share incr intraepithelial lymphocytes
Thickened collagen band > 10 microns
Account for the EPI of Microscopic Colitis and list some clues for its diagnosis
EPI: 10-20% of chronic watery diarrhea
Clues:
F>M
>50 y/o
Nocturnal sx
New or recent changes in medications
Autoimmune diseases (ex: hypothyroidism may lead to 2nd autoimmune process)
What is the first step in management of Lymphocytic Colitis if patient takes NSAID for arthritis? What is a possible complication that can arise? What are some medication alternatives?
Discontinue ibuprofen, add budesonide (80% effective)
9 mg/day for 6-8 weeks; taper 6 mg/d (1-2 weeks), 3 mg/d (1-2 weeks), then stop
60-80% relapse w/ cessation
Alts: Prednisone (Budesonide spares AE’s)
Bismuth
Mesalamine
If patient is counseled to stop smoking bc this poses an incr risk of microscopic colitis, what other medication apart from NSAIDs poses a risk?
*Special Consideration*
Omeprazole
PPI’s ↑likelihood of microscopic colitis
Synergy: Omeprazole + NSAID ↑ risk than either alone
What are the 3 main associations w/ Microscopic Colitis?
1) Smoking: ↑ risk & onset by 10 years early
2) Celiac Disease: 5%, 70x greater risk
3) Medications:
NSAIDs
PPI
SSRI
Anti-Parkinson Meds
*Usually short exposure time*
What type of bowel change calls for an infectious stool study?
Infection would present as diarrhea, not as constipation
What is the best diagnostic test?
What are your suspicions?
60 y/o f px w/ new onset constipation over past 3 days. She notes worsened LLQ pain but w/o F/C. No change in medication. PE reveals focal LLQ tenderness w/ guarding, no rebound. Elevated WBC’s
Abdominal CT scan bc suspicion of diverticulosis from change in bowel habit, leukocytosis & LLQ pain
What does this abdominal CT scan reveal?

Acute Uncomplicated Diverticulosis
Wall thickening, hyperemic bc brighter- w/ fat stranding
↑ density of soft tisue & pericolic fat
If acute diverticulosis becomes complicated, what are 3 possible findings?
Abscess, Fistula, Perforation into abdomen
With dx of acute diverticulitis, broad spectrum antibiotics are initiated w/ what other step in management? Why?
Colonscopy 6-8 weeks after recovery and antibiotic completion to rule out underlying carcinoma
*CI: immediate colonscopy bc risk of perforation
Describe the management of Acute Diverticulosis
NPO initially but bowel rest, later can advance w/ low residue diet (low fiber, fewer leafy greens & fruits bc indigestible and can tax GI)
*No data to support eliminating nuts and seeds*
Is surgery indicated after the first episode of Acute Diverticulitis?
No bc 20% will have recurrence, although segmental resection can reduce frequency of recurrence
How is Complicated Diverticulosis managed? How does it compare w/ uncomplicated disease?
Non-surgical Tx for uncomplicated disease
Complicated Disease (15% of cases)
- Abscess < 4cm: ab’s and low residue diet
- Abscess > 4cm: IR drainage & eventual elective surgery
- Urgent surgery: peritonitis, perforation, medical therapy failure, undrainable abscess, obstruction
Describe the EPI of Recurrent Diverticulitis
Recurrent attacks: 15%
Higher recurrence in the young (<40 y/o)
Recurrent episodes not necessarily more serious
Even after elective resection, recurrence: 10%
When would a diverting colostomy be performed w/ a Hartmann’s pouch? Describe the procedure
Recurrent diverticulosis w/ inflamed abdomen in earlier spot, complicated by perforation. PE may exhibit diffuse abdominal tenderness w/ rebound
Hartmann:
1) Remove colon section w/ active inflammation and infection, though 2 ends not anastomosed
2) Make a blind pouch w/ colostomy bag
3) Reconnect 2 ends and eliminate ostomy AFTER infection passes
How should surgeon proceed if, prior to reanastomosis surgery, colonscopy (to exclude cancer) shows rectum inflamed w/ ulcers?
Continue as planned w/ re-anastomosis-resolves inflammation so no need to delay!
Tx for Diversion Colitis
Stasis changes bacterial flora, deficiency in short chain FA’s, occurs within 3 mo’s
Sx: bleeding, discharge, pain (or asx)
What is the pathophysiology of Diversion Colitis?
Deficiency of short chain FA’s due to diversion of fecal stream, normally absorbed by simple diffusion and ion exchange
Fewer anaerobic flora- lack of CHO and protein metabolites