Chapter Two - Mechanics of breathing Flashcards
(25 cards)
What do we do to get air into the lungs, in general?
Respiratory muscles: diaphragm contracts, expands the chest wall, the pressure decreases around the lung and we suck air into the lungs.
We have movement of fluids, always from high pressure to low pressure
Lungs keep a negative pressure to ensure that the air can come into the lungs
Describe this graph.

Image explains the process of pressure in the lungs when we inspire and expire
X axis = pressure in the lung becomes more negative when we inspire
We measure force in terms of pressure. Essentially how volume changes with changes in pressure.
During inspiration as we breathe in, and move along the x axis on to the right, the pressure decreases and the volume expands, increases
During expiration, the respiratory muscles relax due to elastic recoil, the pressure around the lungs become more positive and the air comes out of the lungs
What do these abbreveations stand for?


Which lung volume and capacities go where?
Some of the air, we can’t get out, and that is the residual volume. Small airways collapse and trap the air there.
Tidal volume = is the volume of air that you breathe in and out as you are sitting = quiet breathing
She will give us the labelled diagram
Inspiratory Reserve volume = this is
Functional residual capacity = is the air remaining in the lung when you expire
What is the average tidal volume?
Average tidal volume = typical = 500 ml = 450 - 550 ml = IMPORTANT to know
Describe the mechanical events that occur that allow air o enter and leave the lungs. How do these muscles (diaphragm and external intercostals) create negative pressure?
The diaphragm contracts and creates negative pressure and sucks air into the lungs. More in detail…
Bucket and pump handle, and abdominal wall contraction: increases the volume and create this negative pressure
Because of the pleura: the rib cage and the lungs expand together
The abdomen is also included in the chest wall
Where is the diagram inserted? How could we describe its movement? How does it expand the chest wall?
The diaphragm = part of the diaphragm inserts on the ribs itself = part of it also lies next to the chest wall which includes the abdomen.
To appose, means to act next to (appositional action)
Movement of the diaphragm is similar to the movement of a french press, it pushes down on our abdomen
Abdomen is stiff if we have abdominal muscles, so the pressure increases, and that increase in pressure moves the rib cage out through this apposition and contact to the chest wall.

What is the role of the abdominal muscles in inspiration? What happens if you don’t have abdominal muscles or a spinal cord injury? Or COPD?
Diaphragm descends and pressure increases , that increase in pressure affects the chest wall through the zone of apposition and pushes it out. ** For inspiration = abdominal are super important because of this concept ! really need to understand the importance of this wall
If you don’t have any abdominal muscles … so high spinal cord injury C3, C4, C5, would mean that the abdomen is not as stiff… so the abdominal contents are pushed down, they don’t push away the ribs and there is no increase in volume
Quadriplegics: looks like they have a big belly, but it’s the abdominals that can’t hold the content in place.
When people have COPD = could have a barrel chest = when hyperventilation happens the air can not get out and the lungs stay bigger
* Pab: pressure abdominal
*Babies’ chest wall is too compliant, that is why they breathe only with their abdomen. We’ll get to that later on in the course

Describe the pressure-volume relationship in the lung.
Compliance/Stiffness:
C=(change in) Volume/(change in) Pressure=V/P
Pressure becomes more negative move right on the x axis and volume increases moving up the y axis.
This is not a linear relationship, it is a sigmoidal curve
If we start at a point, where the lung has much more air in it… the volume does not change much…
***Think of balloon analogy = when you blow into a balloon it’s easier when you start and you can get more air in it… but it becomes much more difficult at the end when it is inflated.
Bottom line: it describes the stiffness of the lung, with we call compliance
** Review the difference between compliance and elasticity
Definition of compliance = how easily something is deformed
At the bottom or the curve: if I get a big volume change for my pressure change = the lung is very compliant = the lung is not stiff. At the top of the curve, the opposite happens: it takes a whole lot of pressure change to do a pressure change.
When the slope of the line is high, the lung is very compliant. It is NOT stiff.

If you slice the lung transversaly, what kind of regional variation in lung volume? With the alveoli? How does the pressure gradient change?
Slice the lung:
The alveoli at the top of the lung have way more air then the alveoli at the bottom of the lung = notice in the image
Because there is more negative pressure at the top of the lung = there is more volume. Effect of gravity.
Like a slinky, it is JUST an effect of gravity. So we can see the gradient of pressure of gravity
Pressure gradient at the top of the lung = top is much less pressure than the bottom of the lung just like there would be a lot less pressure at the top of mount everest than there would be at the beach
Slinky is to understand the space of the coils = which would be similar to the space that is given for the alveoli

How is the periphery of the lung different than the center?
Periphery of the lung is different than the bottom of the lung: the airway tree, the leaves are out at the periphery, and that’s what happens in the lungs. Big airway and alveoli at the outskirts of the larger airway, which is at the bottom and the top, all over the periphery of the lungs.
How is the volume at the top of the lung different than the one at the bottom? Is the negative pressure different too?
Volume at the top of the lung is greater than the volume at the bottom of the lungs.
IMPORTANT: when we breathe in, we create negative pressure, it’s the SAME negative pressure all around the entire lung that we create (so that means that there is a bigger pressure CHANGE at the bottom of the lung, than at the top) = what that means is that when we breathe in = more air will go to the bottom of the lung than the top of the lung, because the alveoli were smaller to begin with and therefore more compliant
Recap = more air to the bottom of the lung, because more compliant and less pressure = they accept the volume more easily

What is the dependant and non-dependant lung? So in this person who is lying on their side, where is the top/non dependant of the lung? Where is the more expanded part of the lung?

Dependant = bottom of the lung
Non-dependant = top of the lung
When you breathe in, more air goes into the dependant part of the lung
If we have someone who maybe has a collapsed lung (collapse alveoli) = we might want to think of a way to lie down , simply physics will maybe help the person breathe
So we might do some breathing exercises lying on that side and then change side to see if we can keep the alveoli open
We see if the action that we took is really working
Non-dependant: It is under right arm
Think about the effect of gravity
The alveoli will be bigger
Where is the more expanded part of the lung? The lateral right side, where the pressure is most and the alveoli are bigger
What is the difference between a standing and a side-lying in terms of difference in the lung volume?

There is a non-dependant and dependant lung, but within each lung, there is also a non-dependant and a dependant AREA
Side-lying position: there is a less big effect of gravity than in a standing position
What are some other situations that might affect lung stiffness?
If the person is a smoker: that will make the lung stiffer. Tar coating sets up an inflammatory reaction in your lungs, the elastic fibers get degraded so the elastic tissue itself is not elastic anymore, there is a lot of air = so it becomes stiffer. This is not important now: more in the second semester.
Balloon analogy: the balloon is hyperinflated, so it is stiff.
Pneumonia: we often call it a consolidation… more fluid in the lungs so it causes more pressure. The interstitium gets filled with pus, so the lung is sort of like a sponge filled with pudding, so the lung gets very stiff/boggy.
*mucus is normal/ pus is not
Atelectasis: it refers to a lack of air in the alveoli. We can have scattered alveoli that are atelectatic .. or we could also have an area. It does not refer to the degree just not enough air. If something is airless … it is stiff → just like the analogy of a long balloon, it is really hard to blow that in. This aspect comes back to remind us that we always need a residual air since…
If we could suck all the air out of the lungs, we could probably never get air back in ever again
What situations might affect the chest wall stiffness?
If the chest wall is stiff, it will not be able to expand as well
People with obesity = have a very stiff chest wall because of all adipose tissue and that makes for a very stiff and hard to breathe
What are the principle determinants of airflow (Poiseuille’s equation)? How do they affect it?
The flow (flow) is related to the pressure (P) change divided by theresistance to air flow (R). The length of our airway tree does not change, what changes is the radius of our airways.. If it gets smaller, it will increase the resistance. To clarify : if the radious gets smaller, creates a huge increase in resistance. The most determinant factor of the air flow in our airways is the radius.
**That equation only goes for laminar flow, not turbulent flow (so not in the trachea or bronchi)

Which factors affect airway radius?
Object in the airway, ex. peanuts, or lego with kids
An allergic reaction
Obesity
MUCUS = cystic fibrosis which means you have an overproduction of very thick mucus and that makes it harder to breathe
-This example is the one that is important
Where is the area in the lungs that has the higher airflow resistance in the tracheal-bronchial tree?
At the periphery = the surface area is so HUGE = and for that reason we have very little resistance at the periphery of the lung. Most of the resistance is at the medium size airways.

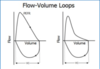
What is spirometry? What does it measure?
Spirometry: breathing test. Deep breath in, and then we blow out as hard and as fast as we can
It measures flow and volume of the lungs
Forced expiratory flow is a big predictor for…
Forced expiratory flow = big predictor of airway disease = the first big curve at the beginning in the expiration
Right graph: curve is very representative of someone who has COPD
Why is surfactant important? What would happend if we did not have any? Use the term radius.
Important because it reduces surface tension
The role of surfactant is to decrease surface tension when the radius gets smaller. Result: the smaller the alveoli gets, the tension reduces and therefore the pressure doesn’t go up. Small alveoli that are not emptying all their air into the larger alveoli
Small alveoli rather than one big: increases surface area: more air exchange area
Surfactant is important because it allows the lungs to increase their surface area so that you have more sites for gas exchange.
Graph: alveoli b will empty all its air into alveoli a… that is a problem… If the alveoli gets small the pressure gets large. In a biological system we have movement of gas from high to low pressure, so from smaller to bigger alveoli

What are some factors that affect the compliance… in the lungs? In the chest wall?
Lung: volume, surface tension, cellular matrix
Chest wall: skeletal system, soft tissue
Why is the information about surfactant and surface tension relevant to a physiotherapist?
Because it would indicate therapy approaches, or what is possibly the problem — e.g. atelectasis?
