Block 3 - Male GU Flashcards
____ is a urethral orifice involving the ventral surface of the penis
Hypospadias
___ is a urethral orifice involving the dorsal surface of the penis
Epispadias
_____ is an abnormally small orifice of the prepuce which interferes with cleanliness and permits the accumulation of secretion and detritus under the prepuce, favoring infection and carcinoma
Phimosis
___ is non-specific inflammation of the glans penis and prepuce. Can be caused by a variety of organisms, including anaerobic and pyogenic bacteria.
Balanopsthitis
____, the accumulation of desquamated epithelial cells, sweat, secretions, and debris is uncircumscribed penises. Eventually leads to phimosis
Smegma
Painful vesicular lesions involving the glans penis and prepuce. Contain clear fluid on an erythematous base.
Herpes simplex
Penile tumor from HPV 6 or 11. Does not result in carcinoma. Most commonly after puberty. Gross morphology shows sessile or pedunculated papillomatous lesions of the coronal sulcus of the inner surface of the prepuce Hyper keratosis, acanthosis, koilocytes, and retention of polarity
Condyloma acuminatum
Cell type and associated disease

Koilocytes
Condyloma acuminatum (HPV 6 or 11)
Dx?

Acute epididymitis
Penile cancer associated indirectly with circumcision and directly with high grade HPV strains. Also related to cigarette smoking.
Squamous cell carcinoma
Condition characterized by a feeling of “worms” in the testicles and infertility.
Variocele
Which side is a varicocele most likely to occur on and why?
Left. Left testicular vein drains into the left renal vein, whereas the right side drains into the IVC. The left side therefore has increased venous pressure.
Testicular cancer occurring in middle aged men. Appears as sheets of uniform polygonal cells with abundant clear cytoplasm, large nuclei, glycogen in cytoplasm, lymphocytes in the stroma. Cut surface shows NO necrosis or hemorrhage, differentiating it from other tumor types. Granulomas form. +PLAP, +KIT

Seminoma
Testicular cancer that occurs in young adult males. Appears as poorly differentiated, pleomorphic cells in cords, sheets or papillary formation. Tumor giant cells and mitotic figures. Most contain some yolk sac and choriocarcinoma cells (mixed). Negative tumor markers unless mixed cells are present. -KIT

Embryonal carcinoma
Testicular cancer occuring in infant male patients. Appears as poorly differentiated endothelium-like, cuboidal, or columnar cells with Schiller-Duval bodies. Primitive, glomerular-like structures that represent endodermal sinuses. +AFP and a1-antitrypsin

Yolk sac tumor
Testicular tumor occuring in young adult males. Appears as cytotrophoblasts and syncytiotrophoblasts without villus formation. Usually small lesions without testicular enlargement. Hemorrhage seen grossly and microscopically. +hCG. Highly aggressive.

Choriocarcinoma
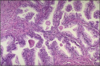
Testicular cancer occuring in all ages. Appears as tissues and cell types from all three germ cell layers with varying degrees of differentiation. Negative tumor markers.
These are ALWAYS malignant in postpubescent males
Mature: all elements well differentiated
Immature (seen below) : incomplete differentiated

Teratoma
Testicular tumor occuring in young adult males. Appearance is variable, but most commonly combines teratoma with embryonal carcinoma. (may see increased hCG is choriocarcinoma elements are present or AFP if yolk sac tumor elements are present)

Mixed tumor
Testicular tumor occuring in older men. Indolent and contains cells resembling secondary spermatocytes.
Spermatocytic seminoma
Non-invasive (in-situ) testicular tumor that is considered a precursor lesion for many invasive testicular tumors. Germ cells are replaced by large tumor cells with clear cytoplasm, enlarged vesicular nuclei, and prominent nucleoli. No spermatogenesis. The basement membrane is hyalinized and thickened. Associated ith reduplication of short arm of chromosome 12.

Intratubular germ cell neoplasia
Mutation associated with intratubular germ cell neoplasia
reduplication of short arm of chromosome 12
Sex cord stromal tumor in males that occurs in early or middle adulthood. May elaborate androgens or both androgens and estrogens. Appears as large, round or polygonal cells with abundant pink or vacuolated cytoplasm and well-defined cell borders. Lipochrome pigment and eosinophilic Reinke crystalloids.

Leydig (interstitial) cell tumor
Sex cord stromal tumor in males that may elaborate androgens or estrogens but most are hormonally silent. Appears as tubules and may resemble rete testis. Tall columnar cells resembling cells of seminiferous tubules.

Sertoli cell tumors (Androblastoma)
Testicular tumor seen in older patients. Large B-cell type or Burkitt. Aggressive.

Lymphoma
An inflammatory conidition of the prostate assocaited with organisms causing UTIs. Direct extension from the urethra via lymphatic or hematogenous spread. Presents with fever, chills, dysuria, and a body, tender prostate.
Acute bacterial prostatitis
A long-standing or recurrent inflammation of the prostate. May be asymptomatic or associated with low back pain and dysuria. Associated with organisms that cause UTI and directly extend via lymphatics or blood.
Chronic bacterial prostatitis
The most common form of prostatic inflammation, with an unknown cause. May be asymptomatic or associated with low back pain but the patient has no history of recurrent UTIs.
Chronic abacterial prostatitis
Nodular thickening of the inner (periurethral) portion of the prostate with some lateral and medial involvement (transitional zone). Incidence increases with age and in blacks. Related to hormone imbalance and androgen sensitized receptors, which increase transcription and cell division when activated. Nodular and enlarged prostate. Micro: hyperplasia of both glandular and stromal elements with glandular papillomatosis.
The patient presents with urinary tract obstruction, frequency, nocturia, difficulty starting and stopping flow, overflow dribbling, dysuria, etc.
Does not illicit an increase in carcinoma.

Benign prostatic hyperplasia
Tx for BPH
5a reductase inhibitor
A noncompliant, hypotonic bladder resulting in hypertrophy of the muscular coat of the bladder (detrusor muscle), usually caused by obstruction of the urethra. The reduced muscular tone makes the bladder difficult to empty and may lead to UTI.

Trabecular bladder
Calcifications seen in BPH
Prostate chips of TURP (transurethral resection of prostate)
The most common cancer in males. Incidence increases in age and blacks. Related to hormonal imbalance with beneficial effects seen with increased estrogen and castration. Most commonly arises in the peripheral aspect of the posterior lobe of the prostate. Patient presents with a stony hard mass, without urinary tract obstruction. Micro: back-to-back glandular proliferation with glands lined by a single layer of cells in varying degrees of differentiation.
Increased activation of PI3K/AKT pathway, BRCA1, and loss of p53 or Rb.

Carcinoma of the prostate
Low or high grade increased proliferation of glands in the prostate. Intact basement membrane. Two cell layers, +p63, +HMWCK. Precursor lesion.

Premalignant PIN (Prostatic Intraepithelial Neoplasia)
Prostatic tumor with malignant (one cell layer) glands mixed with benign (two cell layer) glands.

Adenocarcinoma
Immunohistochemical study for prostatic carcinoma
PSA
Special stains (2) for basal cell layer to determine malignant potential of prostatic carcinoma.
If both are seen, signifies benign tumor.
P63 and HMWCK 34E12
immuno stain for infiltrating prostatic adenocarcinoma
alpha-methylacyl-coenzyme A-racemase
Carcinoma causes ____ bone metastasis, which presents as elevated serum alkaline phosphatase.

Osteoblastic
Extensive carcinoma of the prostate presents as elevated serum ___ phosphatase.
acid
What is the drug therapy for carcinoma of the prostate?
Androgen deprivation therapy. LHRH analogs, inhibition of systemic steroid hormone production
A rare histiocytic disease that can occur in any organ but is common in the GU tract, especially the bladder. Increased incidence in immunocompromised patients and women. Caused by defects in phagocytic or degradative function of histiocytes in response to gram - bacteria, resulting in chronic inflammation and intracellular deposition of iron and calcium, called Michaelis-Gutmann bodies.

Urinary malakoplaskia
Intracellular depositions of iron and calcium as seen in urinary malakoplakia

Michaelis-gutmann bodies
Deposition of parasite eggs in the wall of the bladder causing chronic inflammation. Squamous metaplasia and increased risk of squamous cell carcinoma.

urinary schistosomiasis
reduced sperm count
oligospermia
the absence of sperm in semen
azoospermia
The absence of semen
Aspermia
A defect in meiosis causing a 47 XXY genotype in males. Most common cause of hypogonadism. Mild intellectual impairment. Decreased testosterone causing increased levels of FSH and LH.
Absence or blockage of ejaculatory ducts causes low ___ because secretions from seminal vesicles are blocked. Normal testosterone, LH and FSH.
fructose
Most common reason for premature ejaculation. May/may not occur with erectile dysfunction
psychological
An anorgasmic state with no prior orgasm
primary
an anorgasmic state with history of prior orgasm
secondary
Low testosterone with elevated LH or FSH shows a problem at which organ level?
gonad (primary)
Low testosterone with low LH or FSH shows a problem at which organ level?
Hypothalamus or pituitary (secondary)
A semen analysis shows oligospermia with normal testosterone, FSH and LH. Semen fructose is low. What is the anatomic location of the issue?
Ejaculatory duct obstruction
A semen analysis shows azoospermia with normal testosterone, FSH and LH. A urine sample shows sperm. What is the most likely diagnosis?
Retrograde ejaculation
What cell division process is defective in Klinefelter syndrome?
meiosis
Patient with type 2 diabetes complains of ED. The cause is damage to ___ and ___.
vessels and nerves
A male presents for infertility evaluation. Physical exam includes examination of the testicles. What common infertility etiology is most easily detected with the patient in the standing versus lying position?
Varicocele
which of the following can be associated with an anorgasmic state?
a. psychological
b. diabetes
c. alcoholism
d. pelvic trauma
e. opiate abuse
all of the above
which of the following can decrease libido?
depression
chronic alcoholism and drug abuse
medications
chronic illness
pituitary adenoma
chemotherapy
anabolic steroid use
all of the above
A male patient presents with infertility. His testosterone, LH and FSH levels are normal. His urinalysis is normal and semen analysis shows normal fructose levels but immature spermatocytes. What is the likely diagnosis?
Spermatogenic failure
A patient presents with infertility. His testosterone, LH and FSH levels are normal. Semen analysis shows sperm that are present are of normal maturity and normal fructose levels. Urinalysis is also normal. What is the likely diagnosis?
Ejaculatory duct obstruction (cyst, congenital, etc.)
A male patient presents with infertility. His testosterone levels are normal but LH and FSH are elevated. He also complains of recent weight gain, cold intolerance, and general lethargy. What is the likely diagnosis?
Hypothyroidism
A male patient presents with infertility. His testosterone levels are normal, but LH and FSH are increased. He shows no other symptoms and thyroid hormone levels are normal. What is the likely diagnosis?
seminiferous tubule failure (can be due to mumps, etc.)
