Back Clinicals Flashcards
Slipped or herniated disc
Herniation of the nucleus pulposis through a weakened anulus fibrosus, usually posterolaterally; it commonly puts pressure on the nerve roots or dorsal root ganglion exiting the intervertebral foramen at or below this level, leading to the symptoms of a “slipped disk;” these occur most frequently in the cervical and lumbar regions due to these segments being the most mobile.
Radiculopathy
Compression or lesion of spinal nerve roots
Pinched nerve
Refers to spinal nerves compressed by herniated discs or spondylosis; pain and sensory loss follows the dermatome; motor loss may also occur.
Laminectomy
Removal of one or more laminae of the vertebrae; this is often done to remove a herniated disc.
Lumbar puncture (aka spinal tap)
This procedure is used to gather CSF. To perform a lumbar puncture, the patient is lying on the side with the back flexed (spreads everything out). A needle is inserted between the spinous processes of L3 and L4 or L4 and L5 (In an adult, the spinal cord ends at L1-L2 and L3-L4 in a newborn, infant, or small child). A superficial landmark for finding this point is the supracristal line which runs on a line from the iliac crests and passes through L4’s spinous process
Epidural anesthesia
Injection of anesthetic agents into the epidural space. Usually takes 10 to 20 minutes to take effect and has a direct effect on the spinal nerves; this procedure is often used in childbirth and cesarean sections
Spinal anesthesia
An anesthetic agent is injected directly into the subarachnoid space at the L3/L4 vertebral level, anesthetizes essentially everything inferior to the waist.
Caudal anesthesia
This procedure is done using an in-dwelling catheter in the sacral canal; the catheter is inserted through the sacral hiatus, and the anesthetic bathes the sacral nerve roots.
Spina bifida occulta
This mildest form results in a small separation or gap in one or more of the bones (vertebrae) of the spine. Because the spinal nerves usually aren’t involved, most children with this form of spina bifida have no signs or symptoms and experience no neurological problems.
Visible indications of spina bifida occulta can sometimes be seen on the newborn’s skin above the spinal defect, including:
An abnormal tuft of hair

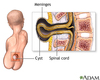
Spina bifida meningocele
In this form, the protective membranes around the spinal cord (meninges) push out through the opening in the vertebrae. Because the spinal cord develops normally, these membranes can be removed by surgery with little or no damage to nerve pathways.
Spina bifida myelomeningocele
In myelomeningocele, the baby’s spinal canal remains open along several vertebrae in the lower or middle back. Because of this opening, both the membranes and the spinal cord protrude at birth, forming a sac on the baby’s back.
In some cases, skin covers the sac. Usually, however, tissues and nerves are exposed, making the baby prone to life-threatening infections.

Scoliosis
Scoliosis is a lateral (toward the side) curvature in the normally straight vertical line of the spine. When a person with scoliosis is viewed from the front or back, the spine appears to be curved.

Kyphosis
Kyphosis refers to the abnormally excessive convex kyphotic curvature of the spine as it occurs in the cervical and/or thoracic region.

Lordosis
The term lordosis refers to the normal inward lordotic curvature of the lumbar spine. A major feature of lumbar lordosis is a forward pelvic tilt, resulting in the pelvis resting on top of the thighs.

What is the Venous Plexus of Batson?
The Batson venous plexus is a network of valveless veins in the spinal canal (epidural space) that connects the deep pelvic veins and thoracic veins to the internal vertebral venous plexuses. Because of their location and lack of valves, they are believed to provide a route for the spread of cancer metastases

