Abdominal Flashcards
List some differentials for acute abdominal pain
Gastric ulcer
Gastroenteritis, UTI, hepatitis, appendicitis, LRTI (non-localised)
NAI (non-accidental injury)
Inflammatory Bowel Disease (IBD)
Diabetic ketoacidosis
Excessive medication, intussusception
Neuroblastoma
Meckel’s Diverticulum
Constipation
What should you ask about in a Acute Abdo pain history?
SOCRATES
Other symptoms: melena, vomiting, haematemesis, PR bleeding, change in bowel habits
Fever, fainting, headaches, chest pain, coughing
Have they tried any new food?
PMH and antenatal hx
DH and immunisation
FH
What should you ask about in a vomiting history?
Frequency, volume and duration
Blood and bile
(also ask about other abdominal symptoms, like stool history, wet nappies etc)
Also ask about travel history
What does bilious vomiting indicate?
Bowel (intestinal) obstruction
Necrotising Entercolitis
Severe gastroenteritis
What does blood in vomit indicate?
Mallory-weiss tear, gastric ulcers etc
What should you ask about if a child has a stool history?
Frequency of stool output
Quality/consistency of the stool (according to bristol stool chart)
Presence of blood
Presence of mucus
What should you look for in an Abdo examination?
Growth deceleration
Delayed puberty
Jaundice
Pallor
Rebound/ guarding/ organomegaly
What are the two types of Inflammatory Bowel Diseases (IBD)?
Crohns Disease and Ulcerative Colitis
What is Tenesmus?
The feeling of needing to go to the toilet without actually having to go to the toilet.
What is the first line treatment for IBD?
5-ASA (Azathioprine) or steroids
What other treatments can be used for IBD?
Methotrexate, Inflixumab and Adalimumab
What are the physical signs of dehydration?
Sunken fontanelles and eyes
Reduced consciousness
Dry mucous membranes
Tachycardia and tachypnoea
Reduced capillary refill time
Reduced Skin turgor
Sudden weight loss
How is gastroenteritis treated in children?
Oral Rehydration Solution (ORS)
What can increase the risk of dehydration?
low birth weight
age <1 year
had >2 vomiting episodes
>5 diarrhoeal episodes in the previous 24 hours
Along with ORS, what other treatments can be suggested for gastroenteritis?
Continue breast feeding and other milk feeds
(Monitor rehydration)
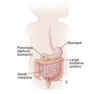
What does X show?

Meckel’s Diverticulum