7.15 Joints of the Hip Flashcards
How many joints are involved in the hip?
One
A ball and socket
Compare the hip ball and socket joint to the one of the shoulder (glenohumeral joint)
The socket is deeper than the glenoid fossa of the shoulder (which is designed for mobility). The hip has much more stability
What are the three components of the hip bone?
- Ileum
- Ischium
- Pubis

What and where is the acetabulum?
It is the socket component of the hip bone

Each component of hip bone (ileum, ischium & pubis) helps form acetabulum.
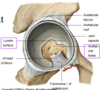
Is all the acetabulum an articular surface?
No
There are 2 parts to the acetabulm
- A lunate surface is the semicircular surface that is the weight bearing region and articular with the femur
- The acetabular notch & fossa are in the centre and are non- articular. This is roughened bone i with exposed trabeculae
Describe the congruence of the three parts of the hip bone
The converge to each contribute (unequally) to the acetabulum.
They converge very well into a ‘Y’ shaped area of congruence and fuse (epiphysis) in late puberty
What is the acetabular notch?
What fills this notch?
A depression in the margin of the acetabulum located anteroinferiorly.
It is bridged by a transverse ligament

What is located deep in the socket and fills irregularities in the hip joint socket/acetabulum?
A fat pad
Intra-articular but extra-synovial fat that has both a nerve and blood supply (source of pain and bleeding) and is also important in spreading the synovial fluid.

Where is the acetabulum ligament coming from?
What function does it serve?
From a depression in the head of the femur (called the fovea). The ligament that goes into the acetabulum.
- It is an intraarticular structure in the joint
- It doesn’t have much other function
Label the major parts of the proximal femur
- Head (with the fovea)
- Anatomical neck
- Greater and lesser trochanter
- The intertrochanteric line
- The shaft

Describe the joint capsule of the hip, especially in terms of where it attaches to
The capsule of the hip bone attaches to the anatomical neck only in utero.
After birth…
- Anteriorly, it migrates distally towards the intertrochanteric line
- Posteriorly it stays near the anatomical neck (migrates slightly distally)

What is contained in the Vascular foraminae of the head of the femur?
These are holes in the bone that enable the passage of blood vessels (around the neck of the femur)
Describe what type of epiphysis the greater and lesser trochanters are
Both trochanters are traction epiphyses which fused and formed due to the pull of muscles/ligaments.
The greater trochanter fuses in mid-teens.

What other kind of epiphysis is present in the head of the femur? Describe its location and formation
A pressure epiphyses - the weight bearing epiphyses also called the capital epiphyses
Dependent on an adequate blood supply getting to that part of the bone.

Describe Perthe’s Disease
When a change (loss) in blood supply potentially affects development of the capital epiphysis of the head of the femur
It causes avascular necrosis of head of femur due to interuption of blood supply
The bone can take between two and five years to re-grow. Perthes’ disease is also known as Legg-Calve-Perthes disease or coxa plana.

Describe the orientation of the large fossa of the head of the femur
It is 2/3 of a sphere
It is directed upwards, medially & forwards (the anterior most part lies outside the acetabulum)
If the anterior most part of the head of the femur lies outside the acetabulum, how is it protected?
By the psoas bursa
It lies deep to the primary flexor of the hip (ileopsoas muscle before articulates to the lesser trochanter).

The roof of the acetabulum is the region that has the thickest cartilage.
Why is this?
This is the primary area of articulation of the head of the femur - where most of the weight bearing is occuring

What enables a greater range of motion of the hip joint?
There is a narrowing in the mid-region of the femoral neck (it is narrower than circumference of head)
This means that there is a range of motion that can be achieved without the bone making contact with the acetabulum and this increasing ROM

How are trabecular patterns of cancellous bone formed?
There is a trabecular pattern of growth that follows the course of stress (weight) lines along the bone. Maximum trabeculae develop along the lines of maximum stess.
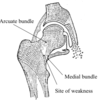
Describe the boney architecture of the head of the femur
In the head of the femur there are two main intersecting trabecular systems:
- SUPERIOR: medial bundle & arcuate bundle – formed due to the compression through head & neck
- INFERIOR: medial bundle & lateral bundle – formed in response to muscle pulls on greater & lesser trochanters

Where is the fracture risk in relation to the trabecular patterns?
Where the two main trabecular patterns intersect
Describe the normal neck-shaft angle of the head of the femur
The angle between the neck of the femur and the head of the femur is about 125 degrees +/- 10 degrees
It is generally a smaller angle for females due to a wider pelvis

Describe the pathology of the angle of inclination of the femur
Increase in the angle = ‘Coxa valga’
Decrease in the angle = ‘Coxa vara’

What is the angle of torsion in the hip joint?
The relationship between the axis of the femoral head and neck and the femoral condyles (the distal end of the femur)
The normal femur has an angle of torsion between 12 and 15 degrees.
It is this angle that causes the anterior part of the head of femur to stick outside the acetabulum

Describe the pathology of the angle of torsion for the femur
- Increase in this angle is termed anteversion
- Decrease in this angle is termed retroversion

Explain coxa vara in adolescence
Coxa Vara = decrease in the angle of inclination

Coxa vara increases stress on femoral neck.
Normally weight-baring forces pass along trabeculae and press on the capital epiphysis to increase stability. But if there is a decrease in the angle of inclination, forces through head of femur may result in the proximal epiphysis not pushing firmly against the head but slides off the remaining part of the head of the femur = ‘slipped capital femoral epiphysis’
Where does the line of gravity pass through at the level of the hip?
What is the implication of this?
At the level of the hip it passes behind the centre of the hip joint
Thus there is a need to reinforce and stabilise the joint in front. The capsule of the hip joint is reinforced ANTERIORLY

What are the 3 ligaments that reinforce the hip joint capsule?
- strong iliofemoral ligament in front projecting far down to the intertrochanteric line (shaped like a V)
- weaker behind pubofemoral ligament
- weaker behind ischiofemoral ligament (this blends with the capsule not directly to femur).

What is the zona obicularis?
An internal lining of fibres forming a ring around the capsule

What is the labrum of the hip joint?
What are the major functions
A (triangular) ring of cartilage that surrounds the acetabulum of the hip.
It has multiple functions:
- Bridges acetabular notch
- Deepens cup & increases surface area
- Creates a suction effect on head of femur (negative pressure)
It is often torn in hip injury

What are the retinacular fibres of the femur?
Reflections of fibrous tissue from capsule to femoral neck contain ‘retinacular’ vessels. The fibres are reflected back along the neck of femur, blended with the periosteum, to the articular margin of the head
Critical blood supply to head of femur.
Across the neck of the femur they are suscptible to injury esp. when the neck is damaged (fracture)

What is the primary hip flexor muscle?
The iiopsoas muscles (inner hip muscles):
- Psoas major
- Iliacus muscle
They attach to the lesser trochanter of the femur

What the extensor muscles of the hip?
Posteriorly:
- The most powerful extensor is gluteus maximus
- The hamstring muscles also contribute to extension.

What is the arrangement of muscles around the neck of the femur? What do they achieve?
The neck is covered by a series of short muscles: act like as rotator cuff muscles (primarily lateral) they run in line with the neck of the femur - push the head of femur into socket

Describe the importance of the gluteus maximus and gluteus medius on posture and locomotion
While walking, the gluteal muscles keep the hips aligned by contracting both sides.
When walking one leg takes all the weight of the body and in order to keep the hips aligned and prevent that weight bearing hip from tilting down, the gluteus muscles contract to pull the contralateral hip down.
They prevent the hip falling away to the unsupported leg during locomotion by contracting on the weight-bearing lip to pull the hip down.

What are the adductor muscles of the hip?
Made up of a big group of adductor muscles
Produce hip adduction – most powerfully from abducted position
Common source of groin pain & pathology – common at bony attachment (osteitis pubis)

What is the main artery that supplies the hip joint?
The main supply to the thigh and hip comes from the profunda femorus artery to femur muscles
aka. deep femoral artery is a branch of the common femoral artery and is responsible for providing
Profunda gives off 2 branches: circumflex femoral arteries (medial and lateral). The medial is more important

Any fracture within capsule and along the neck causes damage to retinacular vessels
What other sequelae can occur?
Muscle spasm particularly of ileopsoas muscle group causing a sterotypic posture: hip joint in external location and shortening of spasming muscles

