196b - Breast Histology, Pathology Flashcards
Lobular Carcinoma in situ (LCIS)
- Type of breast mass:
- Pathologic changes:
- Clinical features:
- Relative risk of carcinoma:
- Type of breast mass: Carcinoma in situ
- Pathologic changes: several possibilities
- Uniform, monomorphic cells
- Bland, round nuclei in loosely cohesive clusters
- Intracellular mucin
- Clinical features: Incidental - no calcifications
- Relative risk of carcinoma: 8-10 fold relative risk
- ~1/3 of women will develop invasive carcinoma in either breast

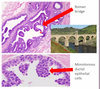
What 2 cell types line breast glands?
- Cuboidal epithelial cells
- Inner layer
- Produce milk
- Myoepithelial cells
- Outer layer
- Squeeze the milk out
- Limiting membrane of breast ducts

Intraductal papilloma
- Type of breast mass:
- Pathologic changes:
- Clinical features:
- Relative risk of carcinoma:
- Type of breast mass: Proliferative without atypia
- Pathologic changes:
- Intraductal - large excretory ducts
- Papillae - fibrovascular stalks
- Mass-forming but benign
- Clinical features: Mass below the nipple, bloody discharge
- Relative risk of carcinoma: 1.5-2 fold relative risk

What is the difference in management of ductal carcinoma in situ (DCIS) vs. lobular carcinoma in situ (LCIS)?
- DCIS - Surgery and radiation
- The DCIS lesion is the one that may become invasive - if you find the DCIS, you know what to remove
- LCIS - Radiation and chemo
- LCIS is basically a marker that something is going wrong in the breast - Location of LCIS does not predict the area that is likely to become invasive
Duct Ectasia
- Type of breast mass:
- Pathologic changes:
- Clinical features:
- Relative risk of carcinoma:
- Type of breast mass: Inflammatory
- Pathologic changes:
- Dilated ducts
- Lymphocytes, plasma cells (one nuclei)
- Pink squamous epithelium instead of cuboidal cells
- Clinical features: Older, multiparous women, nipple pain, retraction, unilateral discharge
- Relative risk of carcinoma: None

How does pregnancy/lactation change the histology of the breast?
More lobules
More acini within each lobule

What is the relative risk of breast lesions in the “nonproliferative” category?
Minimal or no increased risk for developing breast carcinoma
- Acute mastitis
- Duct ectasia
- Fat necrosis
- Simple cysts
- Apocrine metaplasia
- Fibroadenoma
Ductal Carcinoma in situ (DCIS)
- Type of breast mass:
- Pathologic changes:
- Clinical features:
- Relative risk of carcinoma:
- Type of breast mass: Carcinoma in situ
- Pathologic changes: several possibilities
- Architectural: solid, cribiform, papillary
- Comedo: extensive central necrosis
- Low grade (bland, monotonous) or high grade (pleiomorphic)
- Clinical features: Calcifications on mammogram
- Relative risk of carcinoma: 8-10 fold relative risk
- At least 1/3 of women with untreated low-grade will eventually develop invasive carcinoma

What is the relative risk of breast lesions in the “Proliferative without atypia” category?
1.5-2 fold relative risk of developing breast carcinoma in the future
- Usual ductal hyperplasia
- Sclerosing adenosis
- Radial scar
- Intraductal papilloma
Radial scar
- Type of breast mass:
- Pathologic changes:
- Relative risk of carcinoma:
- Type of breast mass: Proliferative without atypia
- Pathologic changes:
- Stellate configuration
- Central nidus of small entrapped glands
- Dilated glands at the periphery with cysts or hyperplasia
- Relative risk of carcinoma: 1.5-2 fold relative risk

What is the relative risk of breast lesions in the “Proliferative with atypia” category?
4-5 fold relative risk of developing breast carcinoma in the future
- Atypical ductal hyperplasia (ADH)
- Atypical lobular carcinoma (ALH)
Sclerosing adenosis
- Type of breast mass:
- Pathologic changes:
- Relative risk of carcinoma:
- Type of breast mass: Proliferative without atypia
- Pathologic changes:
- Lobulocentric proliferation (around a normal TDLU)
- Fibrosis of stroma
- Increased nuber of acini
- Relative risk of carcinoma: 1.5-2 fold relative risk

What kind of breast tissue cells stain brown with smooth muscle myosin immunohistochemical stain?
Outer layer myoepithelial cells

Key differences between atypical ductal hyperplasia and usual ductal hyperplasia?
-
Atypical
- 4.0-5.0 fold increased risk
- Cells are growing in a weird pattern - monotonous, roman bridges, cribiform structures
-
Usual
- 1.5-2.0 fold increased risk
- More cells, but they are in a normal pattern - look like background cells in the terminal duct

Fibroadenoma
- Type of breast mass:
- Pathologic changes:
- Clinical features:
- Relative risk of carcinoma:
- Type of breast mass: Non-proliferative
- Pathologic changes:
- Well-circumscribed
- Biphasic - benign glands and stroma
- Clinical features: Most common benign neoplasm of the female breast; 20-35 y/o, firm, rubbery, mobile, rounded
- Relative risk of carcinoma: None

Apocrine metaplasia
- Type of breast mass:
- Pathologic changes:
- Clinical features:
- Relative risk of carcinoma:
- Type of breast mass: Non-proliferative
- Pathologic changes:
- Apocrine gland: releases some of thier cytoplasmic secretions
- Large, polygonal cells w/eosinophilic, granular cytoplasm
- Small round nuclei
- Clinical features: Pre-menopausal woman, cyclic breast pain, nodularity
- Relative risk of carcinoma: None

Phyllodes tumor
- Type of breast mass:
- Pathologic changes:
- Clinical features:
- Relative risk of carcinoma:
- Type of breast mass: Sarcoma (cancer)
- Pathologic changes:
- Well-circumscribed
- Biphasic - benign glands and stroma
- Clinical features: Rapidly enlarging, 30-50 y/o pt
- Relative risk of carcinoma: Is already carcinoma

What is the functional unit of the breast?
Terminal ductal lobular unit
(This is where most breast lesions arise)

Usual ductal hyperplasia
- Type of breast mass:
- Pathologic changes:
- Relative risk of carcinoma:
- Type of breast mass: Proliferative without atypia
- Pathologic changes:
- Increased number of ductal cells
- Relative risk of carcinoma: 1.5-2 fold relative risk

Fat necrosis
- Type of breast mass:
- Pathologic changes:
- Clinical features:
- Relative risk of carcinoma:
- Type of breast mass: Inflammatory
- Pathologic changes:
- Hemorrhage and neutrophils early
- Macrophages, fibrosis, calcifications later
- Clinical features: Hx of trauma to the breast, calcification on mammogram, hard mass
- Relative risk of carcinoma: None

In general, what are the differences between ductal vs. lobular breast legions?
-
Ductal
- Stronger association with calcifications
- Likely unilateral
- Cells more densely packed, darker purple
- Invasive ductal carcinoma = 70% of breast cancer
-
Lobular
- No association with calcifications
- More likely to be bilateral
- Cells look lighter purple, may have more other stuff in between
- Invasive lobular carcinoma = 10-20% of breast cancer

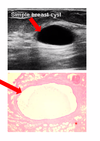
Simple cysts
- Type of breast mass:
- Pathologic changes:
- Clinical features:
- Relative risk of carcinoma:
- Type of breast mass: Non-proliferative
- Pathologic changes:
- Dilated duct with inner luminal epithelial cells, outer myoepithelial cells
- Involves TDLU
- Clinical features: Pre-menopausal woman, cyclic breast pain, nodularity
- Relative risk of carcinoma: None
On H&E stain:
What color is breast stroma?
What color are breast ducts?
Fibrous stroma = pink
Breast ducts = epithelial cells = purple

Invasive Ductal Carcinoma
- Type of breast mass:
- Pathologic changes:
- Clinical features:
- Type of breast mass: Cancer
- Pathologic changes:
- Well developed tubules with low grade nuclei
- 2/3 express ER and PR
- 1/3 overexpresses HER2
- Clinical features: 70-80% of breast cancers
- Hard, palpable, fixed mass

Invasive Lobular Carcinoma
- Type of breast mass:
- Pathologic changes:
- Clinical features:
- Type of breast mass: Cancer
- Pathologic changes:
- Cells don’t stick together (due to E-cadherin mutation)
- Invade individually, single file strands
- Most express ER, PR
- Rarely overexpress HER2
- Clinical features:
- 20% of all breast cancers
- 10-20% are bilateral

Atypical ductal hyperplasia
- Type of breast mass:
- Pathologic changes:
- Clinical features:
- Relative risk of carcinoma:
- Type of breast mass: Proliferative with atypia
- Pathologic changes:
- Cytologic atypia = monotonous cells
- Architectural atypia = arches (Roman bridges), punched out areas (Cribiform structures)
- Ductal epithelial proliferation
- Clinical features: Late 40’s, microcalcifications on mammography
- Relative risk of carcinoma: 4-5 fold relative risk
Atypical lobular hyperplasia
- Type of breast mass:
- Pathologic changes:
- Clinical features:
- Relative risk of carcinoma:
- Type of breast mass: Proliferative with atypia
- Pathologic changes:
- Lobular - uniform, small, dyscohesive cells
- Round nuclei that may be peripheral
- Intracytobplasmic lumens
- Clinical features: Multicentric, bilateral, incidental finding on core biopsy
- Relative risk of carcinoma: 4-5 fold relative risk

What histological changes occur in post-menopausal breast tissue?
More fatty stroma (less fibrous)
Acini are decreased in number, smaller

Acute mastitis
- Type of breast mass:
- Pathologic changes:
- Clinical features:
- Relative risk of carcinoma:
- Type of breast mass: Inflammatory
- Pathologic changes: Neutrophils (multi-lobated nuclei)
- Clinical features: Fever, enlarged, painful, red breast in a nursing mother
- Relative risk of carcinoma: None
