13.3. TB alert 1 Flashcards
Explain what mycobacterium tuberculosis is
- Aerobic
- Predilection for lung
- High lipid content and high mycolic acid content in cell wall
- Likely reason for virulence and resistance
- “Acid-fast bacillus”
- Unable to Gram stain
- Ziehl-Neelsen staining
- Slow growing and long-living
- Group of genetically related mycobacteria
Mycobacterium TB complex
- MTB complex e.g.
- M. TB
- M. africanum
- M. bovis
How can Mtb be spread?
- Airborne droplet nuclei e.g. coughing, singing, communual smoking
- Can remail suspended in the air for hours
- Overcrowded living e.g. prisons
- Oropharyngeal/intestinal deposition
What are the consequences of being exposed to Mtb?
What is a granuloma?
- It is a ccollecction of lymphocytes, macrophages, epithelial cells (if has central necrosis = caseating granuloma)
What symptoms does Mtb commonly present with?
-
Pulmonary
- Cough
- Purulent sputum / haemoptysis
- Breathlessness
-
Extrapulmonary
- CNS / ocular
- Bone / joint
- GI
- Lymph nodes
- Pericardial
-
Constitutional symptoms
- Fever
- Cachexia (extreme ‘weight loss’ and muscle loss)
- Night sweats
How long to symptoms occur for?
- Weeks-months
- Symptoms are progressive
What are the at risk groups of Mtb?
- Immunosuppressed
- Previous close TB contact (esp if in past 2 years)
- Recent travel from high prevalence TB countries
- Prisoners
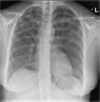
What are common X-ray abnormalities found in Mtb patients?
- Consolidation (air that normally fills small airways in lung are replaced by fluid, pus, blood etc.)
- Effusion (pleural)
- Decreased volume/collapsed lung
- Mediastinal lymphadenopathy (abnormal size or consistency of lymph nodes) e.g. enlarged hilar nodes
- Miliary shadowing
- In picture = bilateral consolidation

What are radiological features of post primary TB (reactivation TB)?
- On CXR (chest C-ray) with past TB contact may have:
- Granuloma
- Apical scarring
- Nodular in upper zones of the lungs
- Consolidation
- Cavitation (Dead, or necrotic, tissue tends to tear and break down e.g. in the lungs)
What is this an example of?

Cavitation in the lungs (Dead, or necrotic, tissue tends to tear and break down)
What is this an example of?

Calcified granulomas
What is this an example of?

Biapical scarring & granulomas
What is this an example of?

Consolidation of the left & right apex
Describe miliary TB
- TB spread via blood (haematogenous spread)
- Often suggests immunodeficiency
What are the symptoms of TB and radiological features?
- In lung
- Widespread fine nodules
- Uniform distribution on CXR
-
Elsewhere
- Liver / spleen in 80-90%
- Kidney 60%
- Bone marrow 25-75%
- CNS disease in 20%
- Patient usually very unwell
- Often have multisystem symptoms
- On CXR has multiple fine nodules throughout the lungs
What are the main sites of extrapulmonary TB?

Explain TB lymphadenitis and diagnosis and treatment
- Cervical LN: scrofula
- Commonest extrapulmonary site
- Cervical chain in 45-70%
-
Presentation
- Slowly progressive LN swelling
- Usually over 1-2 months
- Fever in 20-50%
- Widespread lymphadenitis if HIV / immunosuppression
-
Diagnosis
- Fine needle aspiration or biopsy
-
Treatment
- Standard drug therapy
Explain CNS TB and diagnosis and treatment
- Presentation depends on site
- TB meningitis
- Meningeal symptoms preceded by 2-8 weeks of non-specific symptoms
- Cranial nerve palsies in 40-50%, visual loss, hydrocephalus
-
Diagnose through CSF examination
- High protein, high lymphocytes
- TB bacilli difficult to culture
- Molecular testing: PCR, WGS (see later)
- 12 months of TB treatment needed
- Oral steroids often used
- Significant mortality (if focal neurology or reduced consciousness)
- Other presentations: Tuberculoma, intracranial abscess, spinal cord meningitis
Explain spinal TB and diagnosis and treatment
- More common in thoracic and lumbar vertebra
- 1/3 have evidence of TB elsewhere. 25% have abnormal CXR
- 1/3 have associated psoas abscess
-
Presentation
- Non-specific
- Back pain and systemic symptoms
-
Diagnosis
- Biopsy site and send for AFB
-
Treatment
- May need surgery to stabilise area
- 9-12 months TB drugs (n.b. guidelines say 6 months)
Explain urogenital TB and diagnosis and treatment
- TB spreads via blood to urogenital tract
- Males > females
- Gradual onset
- Average time between pulmonary TB and urogenital TB is 2 decades
-
Presentation
- Dysuria (pain during urination), haematuria, pain
- Fever rare
- Scrotal mass
-
Diagnosis
- Recurrent sterile pyuria
- Urine culture
- Biopsy
-
Treatment
- Standard TB drug treatment
How to diagnose someone with TB using microscopy/culture?
-
Sputum
- Send 3 samples
- Ziehl-Neelsen staining can show Acid Fast Bacilli*
- “Smear positive” = infectious
- Rapid liquid culture (< 2 weeks)
- Solid-medium culture (6-8 weeks)
-
Bronchoscopy
- Not needed if coughing sputum
- May be needed if other differential diagnoses (cancer)
-
Other tissue samples
- Early morning urine (renal TB)
- Pleural biopsy (pleural TB)
- Lymph node biopsy
•Etc
What are the molecular techniques used to diagnose TB?
-
PCR
- Rapid confirmation of presence of MTB complex
- Can identify rifampicin resistance
- Near patient kits can provide result in <2 hours
-
Whole genome sequencing (WGS)
- Identifies species, drug resistance, and can identify transmission cluster
- Important in controlling epidemics
- Compared with traditional contact tracing
- Increasingly quick and affordable
- All positive samples on AFB stain or culture in UK sent for WGS
How can we prevent resistence in TB?
By using multiple drugs to prevent resistance e.g. rifampicin, isoniazid, pyrazinamide
What are the side effects of rifampicin?
- Orange urine, tears
- Rashes and abnormal liver function
- Thrombocytopenia (low levels of platelets)
- Renal failure
- Shock
- Visual disturbance
- Nausea & abdominal pain
Briefly describe rifampicin
- Bactericidal
- Kills active & semi-dormant bacteria
- Has excellent absorption
- Less effective on CNS
What are the side effects of isoniazid?
- Hepatotoxicity
- Nausea and vomiting
- Histaminee foods reactions e.g. fish
- Aplastic anaemia (not enough RBC made)
- Cutaneous hypersensitivity
- Neurotoxicity
Briefly describe isoniazid
- Only active against Mtb
- Kills actively dividing cells
- Good oral absorption
- Metabolised by acetylation
- Therapeutic levels in CSF
- Excreted in urine
What are the side effects of pyrazinamide?
- Hepatotoxic
- Rash
- GI disturbances
- Gout
Briefly describe pyrazinamide
- Kills dormant bacteria
- Inhibits fatty accid synthesis
- Well absorbed
- Also good absorption to CSF
- In hepatic metabolism inhibits renal excretion of uric acid
Briefly describe ethambutol
- Bacteriostatic (capable of inhibiting the growth/replication of bacteria)
- Inhibits arabinosyl transferase
- Absorption can be inhibited by ALCOHOL
- Poor CSF penetration (unless active meningitis)
What are the principles of treatment of tuberculosis?
- Begin treatment with ALL 4 drugs
- DO NOT reduce until 2 months of treatment AND drug sensitivities available
- If FULLY sensitive AND better –> change to isoniazid and rifampicin for 4 months
- If ABSCENT drug sensitivity –> use 3rd agent drug
- Different treatment of CNS affected (usually drugs for 12 months - 2 initial all 4 then 10 months isoniazid and rifampicin)
- Early detection and treatment (completion) is key
Who is more at risk of drug induced liver injury during treatment of Mtb?
- Caucasians
- Older patients
What is IRIS (immune reconstitution inflammatory syndrome)?

Explain infection control in hospitals related to TB
- If able, do not admit to hospital
- Smear positive/suspected pulmonary TB
- nurse in side room vented to outside air, facemask.
- Barrier nursing not necessary for smear negative non MDR TB.
- MDR TB barrier nurse negative pressure side room.
- If HIV negative non MDR TB, usually non infectious after 2/52 treatment.
- If patient found to have TB, risk of infection is low, only those in same room as coughing smear positive case for >8hrs at increased risk.
Explain contact tracing in TB
- Vital in preventing spread of TB
- “Close contact”
- People who have had prolonged, frequent or intense contact with a person who has had infectious (Smear +ve) TB
- If symptomatic close contact
- Assess for active TB: CXR, sputum AFB
- If asymptomatic close contact and <65 years old
- Test for latent TB: Interferon Gamma Release Assay (IGRA) – “Quantiferon gold”
- Consider treatment of latent TB if positive
- Reduces risk of developing active TB by 2/3.
Explain diagnosis of latent TB
- Evidence of positive immune response to TB with normal CXR and no symptoms.
- Immune response assessed by:
- Interferon Gamma Release Assay (IGRA)
- Skin test (Mantoux)
- Immune response assessed by:
Unable to differentiate from those who have cleared bacteria (but immune response remains) and those who have persistent viable bacteria
- Latent TB associated with risk of developing active TB
- Preventative treatment reduces this risk
What are the risks of developing active TB from latent TB?
- Risk of developing active disease increased in:
- Recent (<2 years) contact with infectious (smear positive) individual
- HIV coinfection / immunosuppressed
- Chronic alcohol excess
- Diabetes
- Anti-TNF drug therapy / immunusppressive therapy
- Partial gastrectomy (removal of part of the stomach)
- Balance risk of developing TB with risk of treatment
- Care if frailty, high risk of hepatotoxicity etc
What is chemoprophylaxis?
The use of drugs to prevent disease.
Who are the vulnerable groups of TB patients?
- Children
- New immigrants/refrugees
- Older people
- Homeless, mental health patients
- HIV, Hep B and C patients
- Known TB contacts
- Asian/african groups
- People with co-morbidities e.g. diabetes or immunosuppresed
What is the role of a TB nurse?
To reduce the incidence of TB within the local population
- Case managing TB patients
- Contact screening / incident screening
- New entrant screening
- Working with other professionals
- Involvement with Regional TB networks/ TB regional Board
- Raising awareness and education
How does a TB nurse help patients to be compliant with TB treatment?
- Monitoring the patient at home
- Ensuring patient is taking medication as prescribed
- Maintaining adequate medication
- Monitoring side effects of antibiotics
- DOT / VOT / tablet counts
- Supporting patient attendance with hospital appointments
What are the risk factors of TB?
- Poor housing
- Low incomoe
- Nutrition
- Lack of resources and information
- Immunosuppression, secondary diseases (e.g. HIV)
- Language/cultural barriers
- Overcrowding
- Vitamin D deficiency
- Homelessness
- Smoking
What are the advantages of home visits that TB nurses do?
- Patients talk more about worries and concerns of treatment
- Can identify contacts that patient hasn’t divulged
- Quick access to consultant with issues
- Provide advice and support with treatment and social needs
What are the main symptoms of TB?
- Cough lasting longer than 3 weeks
- Unexplained weight loss
- Fatigue / Feeling unwell / loss of appetite
- Night sweats / Pyrexia (raised body temperature)
- Haemoptysis (coughing up blood)
- Swollen lymph glands
Explain the BCG vaccine
- BCG vaccine helps to protect children mainly against TB Meningitis
- Children may have few symptoms of TB though they can become very ill quickly
- BCG vaccine is 70-80% effective against TB, doesn’t last a lifetime
- Can only be given once, doesn’t always leave scar
