year three - end of life care Flashcards
When is palliative care put in place?
Palliative care put in place when no curative options- symptomatic control, holistic care
What is the Difference between end of life care in hospital vs community?
• Continuity • Knowledge of patient and family • Allows time for conversations and planning
Why do people die today?
o Most common causes of death are cancer and ischaemic heart disease
How do young people die today?
Mostly via accidents - 23% girls - 38% boys
What is the main cause of death in young men aged 15-34?
Suicide
By how much as life expectancy in scotland increased by since 1861?
by 32.3yrs for men and 34.1yrs for women
What are the consequences of unexpected death?
• Causes a profound sense of shock • No chance to say goodbye, or take back hasty words • Accidents might be compounded by multiple deaths, legal involvement or even press coverage • Deaths of children carry an even more profound sense of shock. SIDS has no definite diagnosis and may carry the stigma of parental blame • Terminal care is the last phase of care when a patients condition is deteriorating and death is close • It is often misleadingly only associated with cancer
What does WHO state about palliative care?
: palliative care improves the quality of life of patients and families who face life-threatening illness, by providing pain and symptom relief, spiritual and psychosocial support from diagnosis to the end of life and bereavement
4 bullet points
What does the Scottish Governments Living and Dying Well (2008) state about palliative care?
Palliative Care:
- not just about care in the last months, days or hours of a persons life
- should ensure quality of life for patients and families from diagnosis onwards
- should focus on the person, not the disease
- use a hollistic approach to meet the physical, functional, practical, social, emotional and spiritual needs of patients and carers facing progressive illness and bereavement
What is the role of the GP in palliative care?
To act as a companion
What was the perinatal mortality rate of the 1850s?
>150/1000 live births
What was the highest cause of death in the mid 19th century?
infectious disease - accounted for 1/3 deaths
How do you know when patients need palliative care?
When patient is getting more ill with a chronic condition or they have a life limiting condition
Doctors can use the Supportive and Palliative Care Indicator tool to help in assessment
What should be considered in anticipatory care planning?
o Where do they want to be cared for? o Do they want to be resuscitated in the event of cardiac arrest? o Do they want to die naturally? o Who do they want to be informed of their care and any changes in their condition? o Are they fully aware of their prognosis? o Is their family aware of their prognosis?
What occurs after the patient is put on the palliative care register?
The patients wishes should be sent to the out of hours service so everyone involved in the patient care is aware of the patients plan
What can be used to evaluate how quickly a palliative patients situation is changing?
The palliative performance scale
What symptoms are associated with palliation ?
Pain, anxiety, insomnia, nausea
What must palliative care achieve for patients according to the WHO?
- Provides relief from pain and other distressing symptoms
- Affirms life and regards dying as a normal process
- Intends neither to hasten nor postpone death
- Integrated the psychological and spiritual aspects of patient care
- Offers a support system to help patients live as actively as possible until death
- Offers a support system to help the family cope during the patients illness and in their own bereavement
- Uses a team approach to address the needs of patients and their families, including bereavement counselling if indicated
Who is involved in palliative care?
Macmillan nurses: practical advice, support, financial benefits
- CLAN
- Marie Curie nurses: can come and sit with family and support and give evening care
- Religious or cultural groups
- District nurses
- Occupational therapists: supply equipment and assess patient functionally- hospital bed, commode, air mattress
- Community nurses – evening + all night
- Care manager: organise personal care
What is the DS1500 form?
document stating patient is at the end of their life- opens up available financial support
What is the patients perspective of a good death?
- Pain free death
- Open acknowledgement of the imminence of death
- Death at home surrounded by family and friends
- Aware of death, in which personal conflicts and unfinished business are resolved
- Death as personal growth
- Death according to personal preference and in a manner that resonates with the persons individuality
How should one break bad news?
• Listen • Set the scene • Find out what the patient understands • Find out how much the patient wants to know • Share information using a common language • Review and summarise • Allow opportunities for questions • Agree follow up and support
WHAT NOT TO SAY - “You have cancer.” *gets up and leaves* **cough cough meiklejohn**
What are the reactions to bad news?
• Shock • Anger • Denial • Bargaining • Relief • Sadness • Fear • Guilt • Anxiety • Distress
What are the four stages of grief and loss according to Parkes?
Shock and Numbness
Yearning and Searching
Disorganisation and Despair
Reorganisation and Recovery:
What must be considered with grief?
- Is an individual experience
- Is a process that may take months or years
- Patients may need to be reassured that they are normal
- Abnormal or distorted reactions may need more help
- Bereavement is associated with morbidity and mortality
How many deaths occur in hospices?
15-20%
What is voluntary euthanasia?
The deliberate ending of a persons life with their request
What is non voluntary euthanasia ?
The deliberate ending of a persons life without their request
What is physician assisted suicide?
Physician provides the means and advice for suicide It is illegal in the UK
How many people in the UK ask to die?
3-8% Usually due to unrelieved symptoms or the dread of further suffering
What should be your response if a patient wants to be euthanised?
• Listen • Acknowledge the issue • Explore the reasons for the request • Explore ways of giving more control to the patient • Look for treatable problems • Remember spiritual issues • Admit powerlessness
What are the Just In Case medicines?
• Morphine: pain + breathlessness • Midazolam: agitation • Hyoscine: excess secretions • Levomepromazine: nausea
What is a syringe driver used for ?
Usually initiated when patient struggling to take oral medicine • Mixture of drugs- most commonly morphine + midazolam • 24hrs flow of drugs Subcutaneously • No set maximum dose of morphine- patient given as much as they need
Palliative performance scale

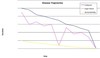
Disease trajectory scale
Old vs New Palliative Care Models

