Tuberculosis Flashcards
What % of the world’s population is infected with TB?
33%
Which mycobacterial species cause TB?
- Mycobacterium tuberculosis
- Mycobacterium bovis
- Mycobacterium africanum
- Mycobacterium microti
All are acid fast bacilli
What is primary TB?
First infection with MTb
Once in the lung, alveolar macrophages ingest the bacteria and the bacteria proliferate within the macrophages
Inflammatory response occurs
Macrophages present the antigen to T-cells
Delayed hypersensitivity reaction occurs which leads to tissue necrosis and granuloma formation
What is a Ghon focus?
The initial site of TB disease
What term is used for a Ghon focus that also involves mediastinal LNs?
Ghon complex
What term is used if a Ghon complex is calcified?
Ranke complex
What % of patients develop active TB following contact with infection?
5%, increasing to 10% within the first year
What is latent TB?
In most people who are infected by mycobacterium spp. the immune system contains the infection and the patient develops cell mediated immunity to the bacteria
= latent TB
What is reactivation TB?
The majority of cases of TB are due to reactivation of a latent infection
How many sputum samples are required to diagnose TB?
3
Patient has TB, what does the chest x-ray show?
Consolidation ± cavitation
Pleural effusion
Widening of medisatinum due to lymphadenopathy
Discuss LN TB
Other than the lungs, LNs are the most common site for TB infection
Most commonly extrathoracic LNs are infected as opposed to intrathoracic or mediastinal LNs
Usually presents as a firm non-tender enlargement of a cervical or supraclavicular LN
On CT the central area can appear necrotic
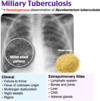
What is miliary TB?
Miliary TB is TB that has spread throughout the body via the blood
This involves the CNS in 20% of cases
Chest x-ray shows multiple nodules which look like millet seeds (hence miliary)
Which stain is most widely used to identify TB?
Auramine-rhodamine - more sensitive than Ziehl Neelsen

Discuss TB treatment
If patient has fully sensitive TB - 6 months of treatment required (unless TB of the CNS in which case its 12mo)
Rifampicin, isoniazid, pyrazinamide, ethambutol
Unwanted effects of rifampicin
Induces liver enzymes which may be transiently elevated in the serum of many patients
Stop the drug if serum bilirubin becomes elevated or if transferases are 3x elevated
Rifampicin can turn body secretions pink
Oral contraceptive will not be effective
Unwanted effects of isoniazid
Very few unwanted effects with this drug
May cause neuropathy due to B6 deficiency but this is rare - common to give pyridoxine to counteract the neuropathy
Can cause hepatitis in <1% but this can be fatal if the drug isn’t stopped
Unwanted effects of pyrazinamide
Hepatic toxicity (rare)
Reduces renal excretion of urate so may cause hyperuricaemic gout
Unwanted effects of ethambutol
Dose related optic retrobulbar neuritis (inflammation of optic nerve) - presents as green colour blindness and reduced visual acuity as well as central scotoma (depressed vision in the centre/ area of focus)
What is mutli-drug resistance in TB?
Resistance to rifampicin and isoniazid
What is extensively drug resistant TB?
Resistance to rifampicin, isoniazid, fluroquinolones and at least one injectable agent e.g. amikacin, capreomycin or kanamycin
How is latent TB diagnosed?
a) Tuberculin skin test - positive result is indicated by a delayed hypersensitivity after 48-72hrs following injection of purified protein derivative. If reaction is very strong, chest x-ray is done to check for active disease **MANTOUX test - may show wheal if patient has had BCG vaccine**
b) Interferon gamma release assays - relies on the fact that T-lymphocytes will release IFN-γ when exposed to specific antigens. Doesn’t distinguish between latent and acitve TB
