Thorax (CXR) Flashcards
1
Q
How are x-rays formed?
A
- photons of energy interacting with the body, essentially producing a shadow of the structures on some detection device
- photographic film: chemical rxn –> silver halide crystals to silver (black); where more x-rays passed through, image was blacker and vv
- negative film using slide projection
- now done on digital detectors and computers
- disadvantages: planar image only, collapses 2D object into 3D; no depth analysis
- only get 3D perspective with another projection e.g. lateral
- advantages: cheap and easy
2
Q
How are chest x-rays taken?
A
- full inspiration
- PA with x-ray to pt back, and heart closest to the film
- ‘hug’ film to move scapulae out of the way
- erect
- to determine blood flow distribution to the lungs
- less blood flow to top of n. lung (larger vessels tf at bottom)
- in LHF, +pulm P, vessels at top are enlarged (pulm vascular distribution)
- to look for pleural fluid, sinks to bases of lungs/pleural cavities
- e.g. pleural effusion
- to determine blood flow distribution to the lungs
3
Q
What determines how many x-rays get through the body?
A
e-density
- xrays interact with electrons
- electrons or close together, greater reaction
- high atomic # things and high concentrations of e- e.g. metals (xrays cannot get through) are white
- air is low e- density, tf black
- fat, soft tissue (muscle, viscera) is grey
- calcium of bone is white
- contrast agents like iodine and barium can be used
- different e-densities side by side = silhouette sign
- same e-densities side by side cannot be differentiated
4
Q
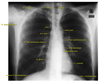
What determines a ‘good’ CXR?
A
- if full inspiration:
- 7 ribs anteriorly in the mid-clavicular line between the top of the chest and the diaphragm
- 11 ribs posteriorly in the mid-clavicular line between the top of the chest and the hemidiaphragm
- silhouette in mid-clavicular line, not impeded by scapular border
- standing straight
- line up spinous processes in the posterior midline to the trachea in the anterior midline
- line up spinous processes with the sternal notch between the medial clavicles
- includes the costophrenic recess, where fluid would be

5
Q
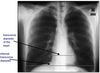
What structures outline the mediastinum on CXR?
A
6
Q
How is heart size assessed on CXR?
A
maximum transverse diameter of the heart must be less than 50% of the maximum transverse internal diameter of the thoracic cavity
(must be erect, PA, full inspiration)
only in adults; does not work if hyperinflated (e.g. smokers, COPD, airway obstruction)
7
Q
How can lung fissures be seen in CXR?
A
In lateral view

8
Q
Pleural cavities on CXR
A
- are only seen if fluid/something is in then
- on R, need to look at lateral view
- fluid sinks, air rises
- fluid open to the atmosphere will be level; fluid not exposed to atomspheric pressure will have a meniscus due to negative intrapleural pressure
- pneumothorax is gas/air in the pleural space that separates the lung from the chset wall
- pleural effusion is an accumulation of fluid in the intrapleural space
