Systems to Cells Flashcards
(161 cards)
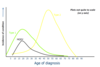
How many ppl in Uk hae diabetes?
4.7 million ppl have diabetes currently
What is the 1st law of thermodynamics?
The First Law of Thermodynamics (Conservation) states that energy is always conserved, it cannot be created or destroyed. In essence, energy can be converted from one form into another.
Diagram of Energy balance

what is energy needed for?
- Cell growth and division
- Building new molecules and replacing old ones
- Movement (muscle contraction is ATP-dependant)
- Breathing, thinking
What is our energy currency?
ATP is an energy currency formed by substrate-level and oxidative phosphorylation.
Memorise ATP energy release diagram

List facts about ATP NOW!
Uhh okay,
- The average human body has 100-250g of ATP
- Daily requirement of ATP is 50-70kg. You make more than your body weight of ATP everyday
- ATP is re-formed from ADP around 1000x a day.
- It is essential for life
- We need to keep replenishing this energy.
what does the complete oxidation og glucose give?
ΔG° = -2840kJ/mol
How is glucose broken down?
Broken down to pyruvate by glycolysis. Under aerobic conditions the pyruvate is converted to Acetyl-CoA and this enters the Krebs Cycle
Under anaerobic conditions, it’s converted into lactate.
can be efficiently stored as starch/glycogen
Is glucose a key energy source?
Glucose is a key energy source.
The brain and nerves have an absolute requirement for glucose for enrgy. So do erythrocytes, tstes and kidney medulla.
What is Whole blood glucose homeostasis?
Whole Body Glucose Homeostasis
- Blood sugar levels kept the same by a range of homeostatic mechanisms
- When in excess, glucose is stored as glycogen in liver and muscle cells or triglytcerides in adipose tissue.
- When levels are low, these tissues become net exporters of glucose/fatty acids
What is Hyperglycaemia vs hypoglycaemia?
Hyperglycaemia is high blood glucose while hypoglycaemia is low blood sugar
How are metabolic pathways involved in glucose metabolism organised?
They’re organised at multiple levels
- System - Human, migrating bird, hibernating brown bear
- Tissue/Organ - Brain, liver, gut
- Cellular - Liver and muscle respond differenlty to high/low glucose
- Subcellular - mitochondria, lipid droplet, cystol
- Genetic - Cells/tissues can change patterns of gene expression in response to nutritional status.
How is glucose level controlled?
Blood glucose is controlled by complex mechanisms
Insulin - rel;eased from pancreatic beta cells when blood glucose inreases
Glucagon - released from pancreatic alpha cells when blood glucose falls.

What does insulin do?
Increasses glucose uptake into fat and muscle cells
Increases uptake of glucose by liver and increases glycogen synthesis in the liver
Inhibits gluconeogenesis in liver
Signals the fed state and the removal of glucose from the blood
What is gluconeogeneis?
Gluconeogenesis is a metabolic oathway that results in the generation of glucose from non-carb carbon substrates such as lactate or amino acids.
What does Glucagon do?
- Stimulates gluconeogenesis
- Inhibits glycogen synthesis in the liver
- Triggers lipid breakdown
- Glucagon signals the release of glucose into the blood.
Homeostasis of Blood Glucose diagram

Where is glycogen mainly stored?
Glycogen is mainly stored in liver and muscle cells
Memorise metabolic pathway of glucose to glycogen

How does Insulin integrate into the glycogenesis pathway.
Insulin turns ‘on’ glycogen synthase and switches off glycogen phosphorylase. Glucagon does the opposite.
Both reactions are energetically favourable - they happen spontaneously
- Allows regulation of enzymes as neeeded
- Allows system to quickly react to changes in blood sugar levels
How do mammals regulate enzymes?
- Changing the rate of biosynthesis/degradation of an enzyme levels by (takes time though)
- Changing the activity of the enzyme (the most common way)
- changing the location of the enzyme
What is reversible covalent modification and how does it regulate key mammalian enzymes?
Commonly used way to quickly regulate enzyme activity in response to a signal (e.g. hormones) is used to use reversible covalent modification. Although this can be include many forms (prenylation, ubiquitation, glycosylation etc.) But most common is phosphorylation
What does phosphorylation involve?
Phosphorylation involves the covalent addition of a phosphate, transferred from ATP by the action of a class of enzymes called kinases.
This is reversible, and the removal of the phosphate is catalysed by a group of enzymes called phosphatases.