Shoulder & Elbow Flashcards
How many degrees do you aim to make the glenoid after TSA?
neutral
In valgus extension overload, when does pain occur (throwing phase)
Deceleration phase
Outcomes of ORIF vs. TEA in displaced intra-aritcular distal humerus fracture in elderly:
TEA has:
- Better 1-2 year outcomes with TEA
- less OR time with TEA
- No difference in ROM
- No difference in re-operation rates
McKee - JSES 2009
Humeral Head Cysts are associated with what kind of soft tissue pathology?
Chronic Rotator Cuff Tear
1st & 2nd line treatments in congenital radial head dislocation
1st: nonoperative
2nd: radial head resection
- Do this as an adult if the patient is symptomatic
- May show some improvement in pain and increased ROM
What type of constraint does a reverse total shoulder arthroplasty have?
Semi-constrained
AC separation classification
I: sprain
II: 25-100% displacement
III: >100% displacement
IV: Posterior
V: >300% through trapezius
VI: Subcoracoid
what are the 3 mechanisms of elbow dislocation?
Axial load: transolecranon dislocation
valgus posterolateral injury (most common)
varus posteromedial injury (coronoid fracture, tear of LCL)
What is the most important structue preventing medial subluxation of the LH biceps?
Subscapularis
Even a partial tear can lead to medial subluxation of the LHB
6 containdications for shoulder arthrodesis
Paralysis of the scapular muscles
Charcot arthropathy
Contralateral shoulder arthrodesis
Ipsilateral elbow arthrodesis
Elderly patient
Progressive neurologic disease
8 indications for shoulder fusion
Post-traumatic brachial plexus injury
Stabilization of paralytic disorder (in infancy)
Insufficiency of deltoid and rotator cuff with arthropathy
Chronic infection
Failed revision arthroplasty
Severe, refractory instability
Bone deficiency following resection of a tumour
Young, manual labourer, with triad of:
- Massive rotator cuff deficiency
- Deltoid muscle insufficiency
- Excessive excision of acromion
Describe the insertion of the biceps on the radial tuberosity. What does each head do?
Long head inserts proximally
Short head inserts distally

Intra-operative options for irreparable rotator cuff tears:
tenolysis to mobilize
graft jacket
partial repair
move footprint
Bail and do tendon transfer
Greatest risk of failure of rotator cuff repair?
Age >65
NOT smoking
How do you get more ER in reverse TSA?
Reduce and get GT to heal
Concurrent tendon transfers (Lat dorsi)
ER osteotomy
Where does a reverse TSA move the center of rotation?
Medial & inferior
Cause of lateral epicondylitis:
Repeated microtraumatic tearing of ECRB
Best repair for coronoid fractures associated with terrible triad
Suture lasso technique
Better than plates/screws
Better than suture anchors
Where does the LUCL usually avulse off of?
Humeral attachment
2 ways to judge reconstruction of humeral head height
- 56mm higher than top of pec major insertion
- 7-8mm higher than GT
What is the most common location for suprascapular nerve impingement?
Suprascapular notch
Most common complications in distal biceps tendon repair/reconstruction?
Lateral antebrachial cutaneous nerve injury
- Most common in both
- new data suggests RARE in 2 incision (0-2%)
Interval for distal biceps tendon repair/
Radial: brachioradialis
Median: pronator teres
(used in both single and 2 incision techniques)
General options for correcting unstable TSA (reverse & anatomic)
Implant:
- Head size: make sure not over-stuffed
- lateralization of implant (more in reverse)
Bony:
Version:
- Make sure it’s correct
- If posterior instability (ie posterior dislocation), dial in more ANTEVERSION
Soft tissue repair:
- Subscap repair (and ensure good force coupling)
- capsule - ± plication
Name 4 contraindications to TSA as per AAOS clinical practice guidelines:
- contraindicated in cases with insufficient glenoid bone stock (glenoid wear to the level of the coracoid)
- rotator cuff arthropathy
- irreparable cuff tears
- deltoid dysfunction
3 complications UNIQUE to reverse total shoulder arthroplasty
Scapular notching
Acromial stress fracture
Dissociation of the glenoid component (glenosphere from head)
What is the most common complication of TSA?
Axillary nerve injury
What direction of displacement of a GT fracture causes the most biomechanical dysfunction?
Posterior
as per Rouleau JAAOS 2016
What has the strongest biomechanical fixation in distal biceps tendon repair?
Endobutton
Final outcome of adhesive capsulitis?
Decreased ROM compared to contralateral shoulder
It will NOT return to normal
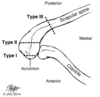
Classification & treatment of acromial stress fracture
Classification by location:
- I: lateral edge
- II: AC joint
- III: Medial to AC Joint
Treatment:
Type I:
- excise
Type II:
- Stable: AC joint resection
- Unstable: distal clavicle excision and fix
Type III:
- Asymptomatic: observe
- Symptomatic: ORIF
*Generally, if Asymptomatic, leave them
How do you classify calcific tendinitis?
Precalcific
Calcific
- Divided into formative, resting, resorptive
Post-calcific
What is a distinctive feature of OA of the elbow?
Maintenance of joint space
However ou do get hypertrophic osteophytes
Describe the Rockwood classification for AC joint separation
Type 1: AC ligament sprain - no displacement
Type 2: AC lig torn, CC lig sprain - displaced <25% CC distance
Type 3: CC distance of 25-100%
Type 4: Displaced posterior through trapezius (Axillary view)
Type 5: CC distance >100% (through deltotrapezial fascia)
Type 6: subacromial or subcoracoid
How do you size the radial head (3 ways)
Size the excised radial head in the measuring device from the set
Align the most proximal portion of the lesser sigmoid notch with the proximal surface of the implant (JAAOS 2014)
- Note that the radial head actually sits 1mm proximal to the coronoid, but they suggest placing the implant at the level of the coronoid to avoid overstuffing
X-ray: medial and lateral joint lines are congruent
Check ROM - too big = abutment of radial fossa of humerus in flexion
4 complications unique to TEA
Bushing wear
Triceps avulsion
ulnar neuropathy
instability (collaterals)
You do a rTSA and need more ER. What do you do?
Lat dorsi transfer
How do you do a load and shift test?
Supine on table.
Bring shoulder to edge of table.
Apply axial load to center humeral head.
Translate HH anterior and then posterior.
Grades:
- Translation to rim
- dislocation with spontaneous relocation
- dislocation without relocation
Outcomes of 1 incision vs. 2 incisions in distal biceps repair:
2 incisions:
greater final flexion strength
less incidence of LABC nerve injury
Treatment/surgical options

Nonoperative if functional.
Operate if non-functional
If unilateral, set in supination of 10-20 degrees
If bilateral:
Fix dominant arm in pronation (30-45 degrees)
Fix non-dominant arm in supination (20-35 degrees)
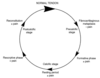
Describe the order of soft tissue disruption in an elbow dislocation
Hori Circle
LCL first
then Anterior/posterior capsule
Then MCL
List 5 options to surgically treat a stiff elbow
osteophyte excision & debridement
distraction interpositional arthroplasty
total elbow arthroplasty
capsular release +/- release of posterior band of MCL indications
musculocutaneous neurectomyindications
Describe Oberlin transfer
Ulnar nerve to upper trunk for upper trunk brachial plexus injury
ie ulnar to musculocutaneous
What has more predictable results in treatment of proximal humerus fractures in the elderly?
Reverse shoulder arthroplasty
2 things that increase MCL (elbow) stress
Increased glenohumeral IR torque
Poor throwing mechanics
Isolated supraspinatus tear: can you do a TSA?
Yes
An isolated supraspinatus tear with no retraction is NOT A CONTRAINDICATION to TSA
10 year revsion free survivorship for TEA in RA?
92%
5 Physical signs of rotator cuff arthropathy
+ ER lag sign
+ Hornblowers
Anterosuperior escape
Pseudoparalysis
Subcutaneous effusion (from loss of containment of capsule and bursa) - there is a name for this sign but I can’t find it - Geissler’s?
What percentage of patients >60 have a rotator cuff tear on imaging?
35-55%
68 year old patient with OA of shoulder and intact rotator cuff. What will give this patient most reliable pain relief?
TSA
TSA > HA in providing predictable pain relief
X-ray for AC joint separation
Zanca
What is the effect of subacromial decompression on rotator cuff repair?
None - results equivocal
What is normal glenoid version?
+5 to -12 degrees of retroversion
Causes of Elbow Contracture? (7)
rauma
surgery
arthritis
cerebral palsy
traumatic brain injury
burns
congenital conditions:
- arthrogryposis
- congenital radial head dislocation
How do you avoid scapular notching in rTSA?
inferior position & inferior tilt of glenosphere
List 5 ways to deal with posterior glenoid bone loss in an arthritic shoulder
Eccentric Reaming
Autograft (humeral head)
Augment (porous metal)
Hemiarthroplasty
Reverse total shoulder Arthroplasty
Which nerve is at risk with an inferior capsular shift (arthroscopic) and how far away from capsule is it at 6 oclock?
Axillary nerve branch to teres minor
12 mm
When do the superior, middle and inferior glenohumeral ligaments provide stability (what angle)?
SGHL: adduction
MGHL: 45 degrees abduction
IGHL: 90 degrees abduction
Think of this when they ask about structures torn in shoulder dislocations

2 absolute and 3 relative contraindications to TEA?
Absolute:
- Active infection (arthrodesis favoured)
- Charcot joint
Relative:
- Poor neurologic control of affected extremity
- Active patient <65 years
- Olecranon osteotomy
Contraindications (4) of rTSA
Deltoid deficiency (axillary nerve palsy)
Bony acromion deficiency
Glenoid osteoporosis
Active infection
After anatomic TSA, how far above the GT should the humeral head be?
5-8mm
Tendon transfer for irreparable subscap tear?
Pec Major transfer
- Pec Major transferred to LT or anteromedial GT
- Must have intact infraspinatus
How do you maximize sensitivity in intraop assessing for infection?
5 cultures at least
Take cultures from seprate regions of both soft tissue and bone
Hold cultures for at least 2 weeks: p.acnes is slow growing
Ultrasound of the implants (to shake off the glycocalyx so that they can culture it)
*No good evidence for intraoperative frozen section (in shoulders)
* If suspecting infection, new data says arthroscopic bx better than aspiration
Outcomes of revision SLAP repair?
Worse than those of primary surgery
New classifiation system of GT fractures
Avulsion: fracture line perpendicular to humeral shaft
Depressed
Split: fracture line parallel to humeral shaft
Why is the anteromedial facet prone to injury in a varus posteromedial instability situation?
It gets sheared off by the trochlea
60% of it is unsupported by the ulnar shaft, making it more prone to injury
Indications for operative management of Hill-Sachs
Classic: >30-40% defect
New: Off-track lesion (engaging) no matter the size
Complications of nonop management of radial head fractures
Elbow stiffness
Insertion of MCL (elbow)
Sublime tubercle of ulnar
In proximity to coronoid
3 options for fixation in distal biceps tendon repair
All suture method
interference screw
endobutton
What open approach do you use for a posterior shoulder dislocation?
Deltopec (go from the front)
But Rouleau says anterior or posterior (JAAOS 2014)
Contraindications to TSA (6)
- insufficient glenoid bone stock
- rotator cuff arthropathy
- deltoid dysfunction
- irreparable rotator cuff (hemiarthroplasty or reverse total shoulder are preferable as TSA causes risk of loosening of the glenoid prosthesis is high (“rocking horse” phenomenon)
- active infection
- brachial plexus palsy
Whatis Friedman’s line?
Line in the plane of the scapular on the axial CT view through the glenoid
Helps you judge version

Elbow pivot shift
How do you do it?
What does it indicate?
(± Arm brought over head so elbow looks like a knee)
Forearm is supinated and a valgus and axial load is applied
Elbow is then brought from full extension into flexion
+ dislocation/subluxation is postiive for PLRI
basically you’re just recreating the PLRI mechanism
What are the primary restraints to posterior humeral subluxation in:
IR
ER
adduction
IR: posteriro band of IGHL
ER: subscap
Adduction: SGHL
Most common nerve injury in shoulder dislocation?
Axillary
What is the main blood supply to the humeral head?
Posterior humeral circumflex artery
Used to be anterior - new data shows posterior
Rehab protocol for TEA for RA? OA?
OA: early ROM at 2 weeks
RA: cast immobilization for 4 weeks, then start ROM
- Delayed ROM protects against wound problems, early loosening, instability (vs early ROM )
Too lateral reduciton/placement of the LT in shoulder arthroplasty will result in a deficit of what motion?
ER
b/c too much tension
Pathophysiology of LIttle Leaguer’s Elbow?
Repetitive contraction of flexor-pronator mass resutling in apophysitis
Name 5 complications with distal biceps tendon repair?
LABC nerve injury (most common)
Radial nerve injury (most severe)
Synostosis
HO
Rerupture
Decreased final strength in flexion/supination
Risk factors for failure of reverse/anatomic TSA
Obesity: they will be in abducted, ER position due to body habitus
Mobility aids: increase shear force through implant
Geyser Sign
Passage of fluid from the glenohumeral joint into the acromioclavicular joint on arthrography is referred to as the geyser sign. It can be seen with chronic rotator cuff tendon tear or after injury of the acromial undersurface during surgery.

What ligament do you release in surgical release of stiff elbow to gain flexion?
Posterior band of MCL
Stages of Frozen Shoulder
1: freezing:
- inflammation & pain
- Lasts 3-9 months
2: Frozen
- profound capsular stiffness & limited ROM
- Lasts 3-12 months
3: Thawing:
- Gradual, spontaneous improvement in shoulder motion and function
- Lasts 1-3 years
Best places for fixation on glenoid side in arthroplasty (doesn’t matter what kind of arthroplasty)
Lateral border of scapula (inferiorly): most important
Base of Coracoid
Center of Glenoid
What is a positive Gagey?
Passive abduction greater than 105 degrees.
Indicates inferior laxity.
Indications for fixation of GT fracture?
5mm displaced
argument for 3mm displaced in a young, healthy overhead worker
(Rouleau JAAOS 2016)
Classification of SLAP tears
I: labral fraying
II: biceps tear
III: Bucket handle
IV: bucket handle with biceps torn off
What phase of throwing is the rotator cuff most susceptible to tension failure? Why?
Deceleration phase
It is the main decelerator of the shoulder and undergoes most eccentric tension during this phase
What is the loss of elbow flexion and supination strength in a proximal biceps rupture
What happens in repair?
Flexion: negligible
Supination: 10-20%
No significant difference with repair
Risks of failure in bankart repair:
Age
Contact Sports
Glenoid bone loss (bony bankart)
Hill Sachs lesion
Describe the instability severity index score (ISIS)
Determines appropriateness of soft-tissue arthroscopic vs. bony repair open in shoulder instability
Age at surgery
>20: 0
Degree of participation in sports (pre-op)
Competitive: 2
Recreational or non: 0
Type of sport (pre-operative)
Contact or forced overhead: 1
Other: 0
Shoulder Hyperlaxity:
Hyperlax either ER >85 with arm at side or + Gagey: 1
Normal: 0
Hill Sachs on AP:
Visible on ER: 2
Not visible on ER: 0
Glenoid loss of contour on AP
Loss of contour: 2
No lesion: 0
Total = 10
= 6: acceptable recurrence risk of 10% with arthroscopic stabilization
>6: unacceptable recurrence risk of 70% and should undergo open surgery (Latarjet)
What is the primary stabilizer of valgus stress to the elbow
Anterior band of the anterior bundle of the MCL
Complications from surgical fixation of radial head
Pain
Instability (PLRI)
Proximal radial migration
Decreased strength (including grip)
Cubitus valgus
HO
Post-traumatic OA of the trochlea-olecr
7 Risk factors for GH dislocation post rTSA
- Irreparable subscapularis (strongest risk factor)
- Proximal humeral bone loss
- Previous failed arthroplasty
- Proximal humeral nonunion
- Fixed GH dislocation preop
- Massive rotator cuff tears with pseudoparalysis
- Excessive humeral retroversion >10 degrees
*note: inflammatory arthritis is NOT a risk factor*
Complications of shoulder hemiarthropalsty (5)
Progressive glenoid arthrosisRisk:
Tuberosity displacement/malunion
Repositioning of tuberosity with bone grafting
Joint overstuffing
Sucutaneous (anterosuperior) escape
Normal acromiohumeral interval (AHI)
8-12mm
Name 2 types of shoulder hemiarthroplasties in terms of head shape:
Standard humeral head
Extended coverage humeral head
- used for rotator cuff arthropathy: the head sits in the acetabularized acromion

How much correction can you safely achieve with eccentric reaming of a retroverted glenoid in TSA?
Patient >40 years old, post-shoulder dislocation, cannot raise arm? Best test? What are you looking for?
MRI shoulder
For ?massive rotator cuff tear
patients >40 with shoulder dislocation have 35-85% rate of massive rotator cuff tear
In unconstrained TSA for proximal humerus malunion, what concomitant procedure provides worse outcomes?
Tuberosity osteotomy (ie for malunited tuberosities)
OK to insert the humeral stem eccentrically/nonanatomically
What are the risks and benefits of lateral decubitus vs. beach chair position in shoulder arthroscopy?

List 7 factors that predict failure of operative Rotator Cuff Repair
Age (>60-70)
Retraction
Muscle atrophy (Tangent sign)
Fatty Infiltration (Goutallier)
Tear Size
Smoker
Diabetic
Name the classification systems (x2) for elbow RA. Describe both
Larsen & Mayo
Larsen:
Stage I: soft tissue involvement, normal xrays
Stage II: periarticular erosions & mild cartilage loss ± osteopenia
Stage III: marked joint space narrowing
Stage IV: progressed erosions past subchondral plate
Stage V: Loss of joint space contour
Mayo:
I: Soft tissue swelling and periarticular osteopenia. Generally normal x-rays
II: Mild to moderate joint space narrowing. Synovitis recalcitrant to NSAIDs
III: Thinning of the joint space contours
IV: Extensive articular damage

Should you do routine acromioplasty in RTC repair?
No - routine acromioplasty non-requied
moderate evidence
AAOS CPG 2010
What treatment is contraindicated in cuff tear arthropathy?
Anatomic total shoulder arthroplasty
Plan for infected TSA 4 weeks out?
Open I&D
May retain implants when acute (
However staged revision is always a safe answer
4 signs of a posterior shoulder dislocation in brachial plexus injury
- asymmetry of skin folds of the axilla or the proximal aspect of the arm (anterior shoulder crease)
- apparent shortening of the humeral segment
- a palpable asymmetric fullness in the posterior region of the shoulder
- a palpable click during shoulder manipulation
(doesn’t include decreased ER bc that is also a sign of the brachial plexus injury)
Treatment for staph epidermidis or p.acnes infection in TEA?
2 stage revision
Will lead to persistent infection if no explant and recurrence if 1 stage revision
In partial distal biceps tear, where is the tear located?
Radially - it peels off
What is a terrible triad injury of the elbow?
Elbow dislocation
coronoid fracture
radial head fracture
(DOES NOT include LCL injury)
Average medial to lateral distance of supraspinatus footprint on GT?
14-16mm
Essential lesion for PosteroMEDIAL rotatory instability
LUCL rupture
anteromedial coronoid fracture
(NO radial head fracture - distinguishes it from PLRI)
Position of Shoulder Arthrodesis
30/30/30
(flex/abd/IR)
Most common site of PIN compression
Fibrous bands of supinator (distal edge)
What must you check for in a patient suspected of medial epicondylitis?
Ulnar neuritis (40%)
MCL injury
First line managmenet for post-traumatic elbow stiffness?
Progressive static splinting
Conceptually, how does a reverse shoulder arthroplasty work?
Provides a fulcrum for the deltoid to work
4 releases with subscap release (open)
(1) its superior margin from the coracoid
(2) the posterior surface from the anterior capsule and scapular neck
(3) the inferior border from the axillary nerve and circumflex vessels
(4) the anterior surface from the conjoined tendon.
What is the majority of motion GAINED from rTSA? Lost?
Gained: forward flexion
Lost: ER/IR
Plan for infected TSA 3 months out?
Explant + staged revision + abx
± one stage
Must explant if chronic infection >6 weeks
7 radiographic findings in rotator cuff arthropathy
acromial acetabularization (true AP)
femoralization of humeral head (true AP)
asymmetric superior glenoid wear
lack of osteophytes
osteopenia
“snowcap sign” due to subchondral sclerosis
anterosuperior escape
2 reductio maneuvers for luxatio erecta
Traction - counter traction
2 step
- Convert to anterior-inferior dislocation by pulling laterally
- Then do regular reduction
What is the initial treatment for a symptomatic patient with a partial RTC tear?
exercise and NSAIDs
AAOS CPG 2010
What is the primary stabilizer against varus stress of the elbow?
Lateral ulnar collateral ligament
Pseudoparalysis is a sign of what shoulder pathology?
Cuff tear arthropathy
Most common mechanism for posterior shoulder dislocation?
Flexion, adduction, IR
Therefore SGHL is most important stabilizer in this position
(Rouleau JAAOS 2014)
Name 3 primary and 3 secondary static stabilizer of the elbow
Primary:
- Ulnohumeral articulation (coronoid)
- LCL
- MCL (anterior band)
Secodary:
- radiocapitellar joint
- capsule
- common extensor and flexor origins
Findings in Panner’s disease (OCD elbow)
Fragmentation of the capitellum
enlargement of radial head
Premature distal humeral physeal arrest
degenerative changes leading to incongrity between radiocapitellar joint
Rate of rotator cuff tear post shoulder dislocation age >40? >70?
Age >40: 55%
Age >70: 100%
Check for this - it’s NOT an axillary nerve injury
Name 5 things that decrease MCL strain (elbow)
Decreased throwing velocity
Trunk-scapular kinesis
Scapular protraction/retraction
Forearm pronation
Dynamic flexor-pronator stabilization/contraction
Which part of the MCL (elbow) is tight in flexion?
posterior bundle
PAL: same as in ACL
2 surgical approaches for distal biceps rupture. What is gold standard?
1 incision
2 incision - considered gold standard now
Name 3 arthroscopic techniques to help repair large rotator cuff tears:
Margin convergence
Anterior interval slide
Posterior interval slide

Complication rate for TEA done for RA?
High: 14% overall
Higher with OA: 25-43%
What soft tissue structure can be injured in valgus extension overload?
MCL of elbow
Main primary restraint to posteiror shoulder dislocation:
Flexion, adduction, IR
Abduction, IR
Abducted, ER
Flexion, ADDudction, IR:
- SGHL, CHL
Abduction, IR:
- posterior band of IGHL
Abducted, ER:
- subscap
What phase of throwing exerts the most stress on the MCL (elbow)
late cocking/early acceleration
How do you perform a reduction of a posterior shoulder dislocation?
Traction (Stimson method)
or
Manipulation: (see below)
(JAAOS 2014)
Two operators are needed for the reduction maneuver.
The physician forward flexes the shoulder to 90° then adducts and internally rotates the arm to disengage the humeral head from the glenoid rim.
The assistant maintains cross-body traction while the physician applies gentle, anteriorly directed pressure to the posterior humeral head.
Finally, external rotation can be attempted to complete and confirm reduction
Greatest direction of loss of ROM in frozen shoulder?
ER
essential lesion in adhesiv capsulitis involves CH ligament/rotator interval
Valgus elbow instability is indicative of what type of instability pattern?
Valgus posterolateral instability
Suggests rupture of LUCL for sure (±MCL)
(JAAOS 2015)

Initial Managemnet of adhesive capsulitis?
gentle, painfree stretching (doesn’t need to be aggressive)
Microscopic evaluation of lateral epicondylitis shows what?
Angiofibroblastic hyperplasia
disorganized collagen
For glenoid component in anatomic total shoulder arthroplasty, is peg or keel biomechanically superior?
Peg
List 6 predictors of successful non-operative Rotator Cuff Tear management
Female
Good scapulothoracic motion
Older age >65
Low demand
Higher baseline QOL scale
Realistic patient expectations
Medial to lateral footprint size of the supraspinatus footprint?
11-14mm
You want to relocate a dislocated shoulder, what kind of anesthesia do you use?
Intra-articular block with lidocaine
Intra-arrticular block should be first, with conscious sedation reserved for difficult reductions
Intra-articular block shows:
- same degree of analgesia
- Same success rate
- Lower cost
- lower time in ER
- Lower overall complications
JAAOS 2014
Outcomes of TSA:
10 year survival
Pain vs. Hemi
ROM
- pain relief most predictive benefit (more predictable than hemiarthroplasty)
- reliable range of motion
- good survival at 10 years (93%)
- good longevity with cemented and press-fit humeral components
- worse results for post-capsulorrhaphy arthropathy
Outcomes post arthroscopic RTCR of 6 weeks immobilization vs. early ROM?
equivalent
Prior to reverse TSA, you want an MRI, why? 2 reasons:
Intergrity of rotator cuff
Fatty infiltration of the muscles (including deltoid)
What 2 ligaments mark the superior border of the subscap?
Coracohumeral ligament
superior glenohumeral ligament
GT displacement/malunion in what position has a poor prognosis, independent of amount of displacement?
posterior
Most common nerve complication after distal biceps tendon repair?
Lateral antebrachial cutaneous nerve (for both approaches)
radial is most severe
Where is the center of rotation moved in a reverse TSA?
medial and inferior
Major radiographic finding of inflammatory arthritis of elbow (x2)
Erosive arthritis with significant bone loss
Loss of joint line
Major sequelae of hypotensive episodes in semi-upright shoulder arthroscopy?
Asystole
ishaemic brain injury
ischaemic spinal cord injury
Name 5 shoulder reduction techniques
What’s the best?
Hippocratic
- Pull & adduct arm with foot in armpit
Kocher’s
- Arm at side, 90 @ elbow, pull and ER –> IR
Milch
Stimson
- Hang arm with weights while prone
Matsen Traction-Counter traction
- With a sheet
Eskimo
Scapular Manipulation
FARES: (Fast, Reliable & Safe)
Adduction with elbow extended. Short vertical oscillating movement and bring arm to abdcution and ER. Should reduce around 120 abduction

3 options for rotator cuff arthropathy
Non-operative management
Reverse total shoulder arthroplasty
Extended surface head hemiarthroplasty
4 risk factors or poor outcome following lat dorsi transfer for irreparable posterosuperior RTCT?
Nonsynergistic action of the transferred muscle
Fatty atrophy of the supra/infraspinatus muscles
Deficieincy of Subscap
Deltoid weakness
Name 4 indicators of an irreparable rotator cuff tear
1) Superior displacement of the humeral head (AHI
2) Fatty infiltration of the rotator cuff muscles (Goutallier stage 3-4)
3) Increased duration of the tendon tear
4) Profound external rotation weakness.
Because they lead to poor prognoses post-op
Name the signs of a preganglionic brachial plexus injury:
Root avulsion, so:
winged scapula (long thoracic nerve)
absent serratus anterior (long thoracic)
absent rhomboid (dorsal scapular nerve)
rotator cuff (suprascapular nerve)
latissimus dorsi (thoracodorsal nerve) function
Horner’s syndrome (sympathetic chain)
elevated hemidiaphragm (phrenic nerve).
Posterior shoulder dislocation: what is the rate of concomitant surgical neck fracture?
50%
How do you prevent cerebral hypoperfusion in shoulder arthroscopy/open procedures (especially with beach chair)
sBP >90mmHg
Max decrease of sBP & MAP
Post shoulder reduction rehab program (1st time dislocation - traumatic)
Immobilize minimum 3-4 weeks
Anterior: no ER past neutral
Posterior: No IR past neutral
What is the most common cause of TSA failure?
glenoid component loosening
Name 2 ways of judging version in shoulder reconstruction
- Transepicondylar axis
- Pre-op planning
- Jig
5 signs that radial head dislocation is congenital
Bilateral
non-traumatic
posteriorly dislocated
convex radial head
hypoplastic capitellum
Associated with other congenital anomalies (achondroplasia)
Difficult to reduce
associated with bowing and shortening of the radius
may be asymptomatic
Patient with Post op shoulder surgery pain. He had an intra-articular local anesthetic pump. Dx?
Chondrolysis secondary to local anesthetic infusion
Risk factors for posterior shoulder dislocation:
Epilepsy
Excessive Glenoid retroversion
Excessive humeral retroversion
Reverse hill-sachs
In valgus extensio overload, where are the osteophytes?
Posteromedial olecranon fossa
2 techincal factors that place RTC tendons at risk during TSA arthroplasty
Too distal of a head cut
Head cut too retroverted

5 risk factors for adhesive capsulitis (Frozen shoulder)
Diabetes
Thyroid disease (autoimmune etiology)
Previous surgery (lung/breast)
Prolonged immobilization
Extended hospital stay
Indications for hemiarthroplasty (4)
Primary arthritis if:
- Rotator cuff is deficient
- Glenoid bone stock is inadequate
- Risk of glenoid loosening is high (young, active, labourer)
Rotator cuff arthropathy
- Hemiarthroplasty > rTSA if able to achieve forward flexion >90 degrees
Osteonecrosis without glenoid involvement
Proximal humerus fractures
Cause of acromial stress fracture:
Overtension of the deltoid
3 Radiographic signs of high-riding humerus (RTC arthropathy)
Decreased acromiohumeral interval (
Break in Shenton’s line
Acetabularization of the acromion
Also: Femoralization of the humeral component: rounding off of the GT
What is the best surgial technique for MCL reconstruction of the elbow?
Humeral docking via flexor pronator split, no ulnar nerve transposition
better outcomes and complication rates
biomechanically stronger
95% strength of native ligament
+ elbow varus stress test is indiative of what pathology?
posteroMEDIAL rotatory instability
Treatment for shoulder tuberosity malunions greater than and less than 1.5cm
Less than 1.5cm: arthroscopic vs. open acromioplasty (to prevent impingement) and tuberoplasty
More than 1.5cm:
Large fragment: tuberosity osteotomy
Small fragment: tuberoplasty
JAAOS 2014
T/F
Surgical resection/management of calcific tendinitis results in higher risk of rotator cuff tear?
False
very low rates of tendon injury/compromise post surgical resection
What are ywo options when you have excessive glenoid retroversion in anatomic total shoulder arthroplasty?
Build up posterior glenoid via bone graft/augments
eccentrically ream the anterior glenoid (if there is enough bone stock anteriorly)
Name 2 ways to get more ER with a reverse total shoulder arthroplasty:
Concomitant latissimus dorsi transfer
ER ostoetomy of the humerus
7 indications for rTSA
Rotator cuff arthropasthy
Pseudoparalysis
Antero-superior escape
Acute 3-4 part PHF
Where GT has poor healing potential
RTC insufficiency equivalent
- Nonunion or malunion of the tuberosity following trauma or prior arthroplasty
Failed arthroplasty
RA
- If bone stock is sufficient
Functional ROM of the elbow
30-130 extension/flexion
ie the range the MCL is most important
Tendon transfer for irreparable supra and/or infraspinatus tear?
Lat dorsi transfer: for infraspinatus irreparable tear (ER lag)
Lat dorsi and/or teres major is transferred to GT
Must have intact subscap
3 ways to help mobilize a retracted tendon while repairing RTC:
Maximum relaxation/paralysis
Change position of arm
Tenolysis - thorough superior, inferior, medial, lateral
Incidence of the following in luxatio erecta:
cuff tears/GT fractures
Neurologic injury
vascular injury
cuff tears/GT fractures: 80%
Neurologic injury: 60%
vascular injury: 39%
T/F
MGHL is absent in 60% of shoulders?
False
MGHL is absent in 30% of shoulder
What are the essential lesions ofr varus posteromedial elbow instability?
What happens if it’s not diagnosed/treated early?
Coronoid fracture (anteromedial facet)
LUCL injury
Can lead to rapid onset of ulnohumeral arthritis
IN Bilatera elbow fusion, what angles do you fuse at?
Dominant arm: >90 deg
Non-dominant arm:
