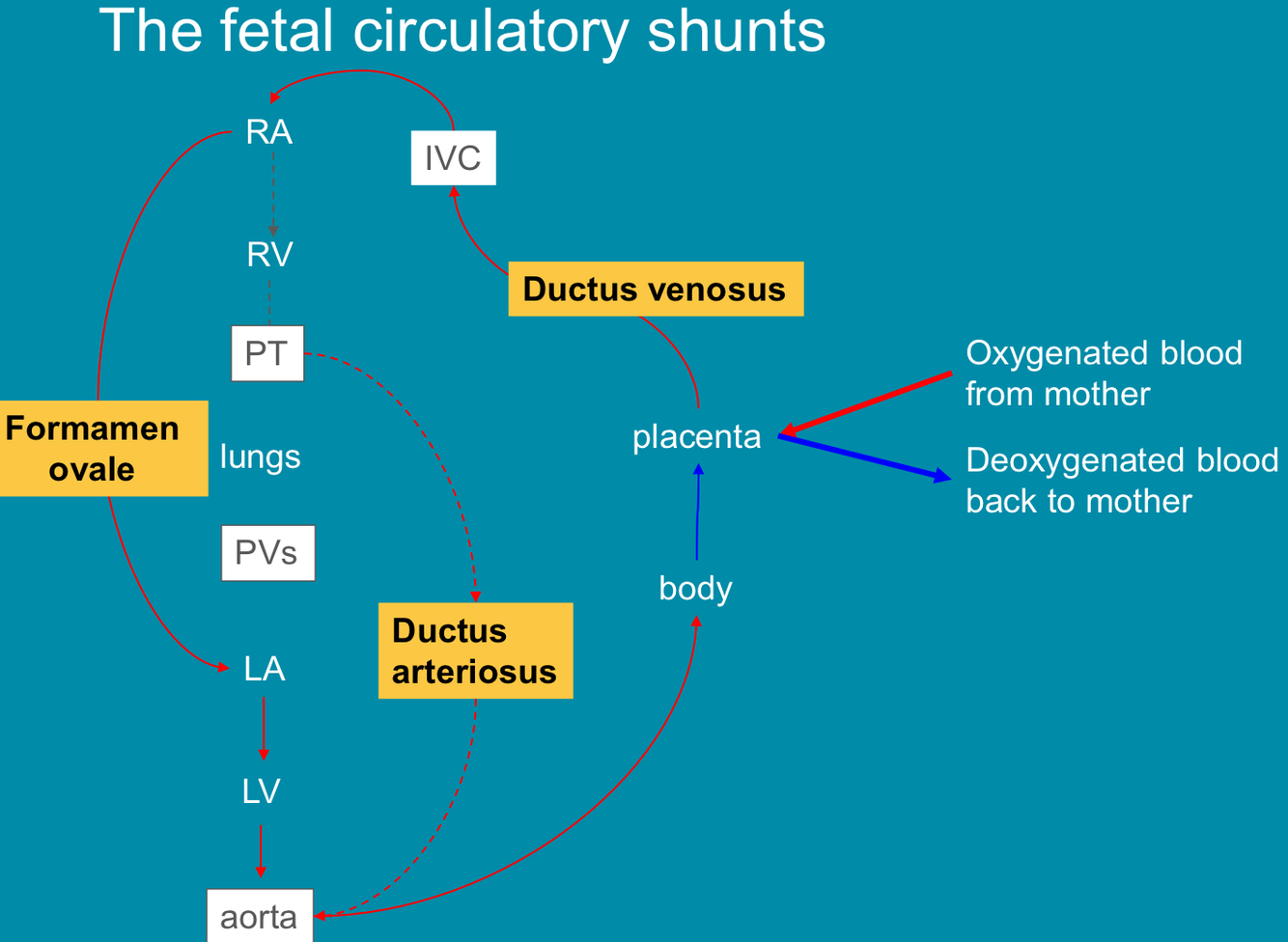
Oxygenated blood carried via the umbilical vein
• Deoxygenated blood carried via the umbilical arteries
pO2 approx. 4kPa compared to normal adult pO2 of 11 – 13kPa
– Fetal haematocrit is increased over that in the adult
– 0.513 – 0.56 l/l cf 0.4 – 0.54 l/l in adult males
– Fetal Hb = 166 – 175g/L cf , 95 – 140 g/L at 2 years and 130 – 180 g/L in adult males
• Increased maternal production of 2,3 DPG
– Secondary to physiological respiratory alkalosis of pregnancy
- Fetal haemoglobin (
- Predominant form from weeks 12 – term is HbF
- 2 alpha subunits plus 2 gamma subunits
- Greater affinity for oxygen because it doesn’t bind 2,3-DPG as effectively as HbA)
- Double Bohr effect (• Speeds up the process of O2 transfer
- As CO2 passes into intervillous blood, pH decreases • Bohr effect
- Decreasing affinity of Hb for O2
- At the same time, as CO2 is lost, pH rises
- Bohr effect
- Increasing affinity of Hb for O2)
CO2 Transfer
• Maternal physiological adaptation to pregnancy • Progesterone-driven hyperventilation
• Hence lower pCO2 in maternal blood
• Concentration gradient
- Double Haldane effect
- As Hb gives up O2, it can accept increasing amounts of CO2 • Fetus gives up CO2 as O2 is accepted
- No alterations in local pCO2
Draw a diagram showing fetal circulation
Fetal response to hypoxia
• Fetal heart rate SLOWS in response to hypoxia to reduce O2 demand
• Fetal chemoreceptors detecting decreased pO2 or increased pCO2
– Vagal stimulation leading to bradycardia
– cf adult where vagal inhibition leads to tachycardia
• Chronic hypoxaemia
– Growth restriction
– Behavioural changes
• Impact on development
- Hormones necessary for fetal growth
- – Insulin
– IGF II nutrient independent, dominant in first trimester
– IGF1 nutrient dependent, dominates in T2 and T3
– Leptin (Placental production)
– EGF, TGFa
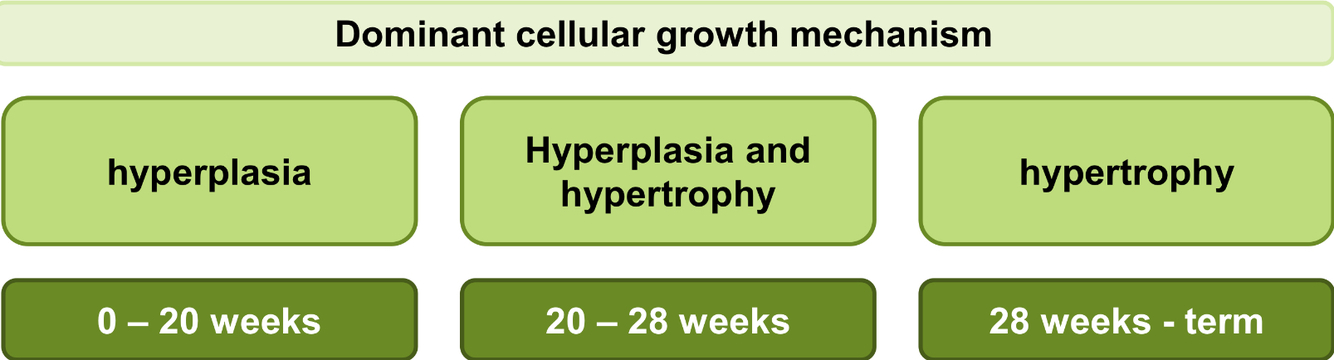
Effects of nutrition on fetal growth during pregnancy
- Malnutrition can cause ? growth restriction
- State the dominant cellular growth mechanism during pregnancy
- symmetrical or asymmetrical
- Image
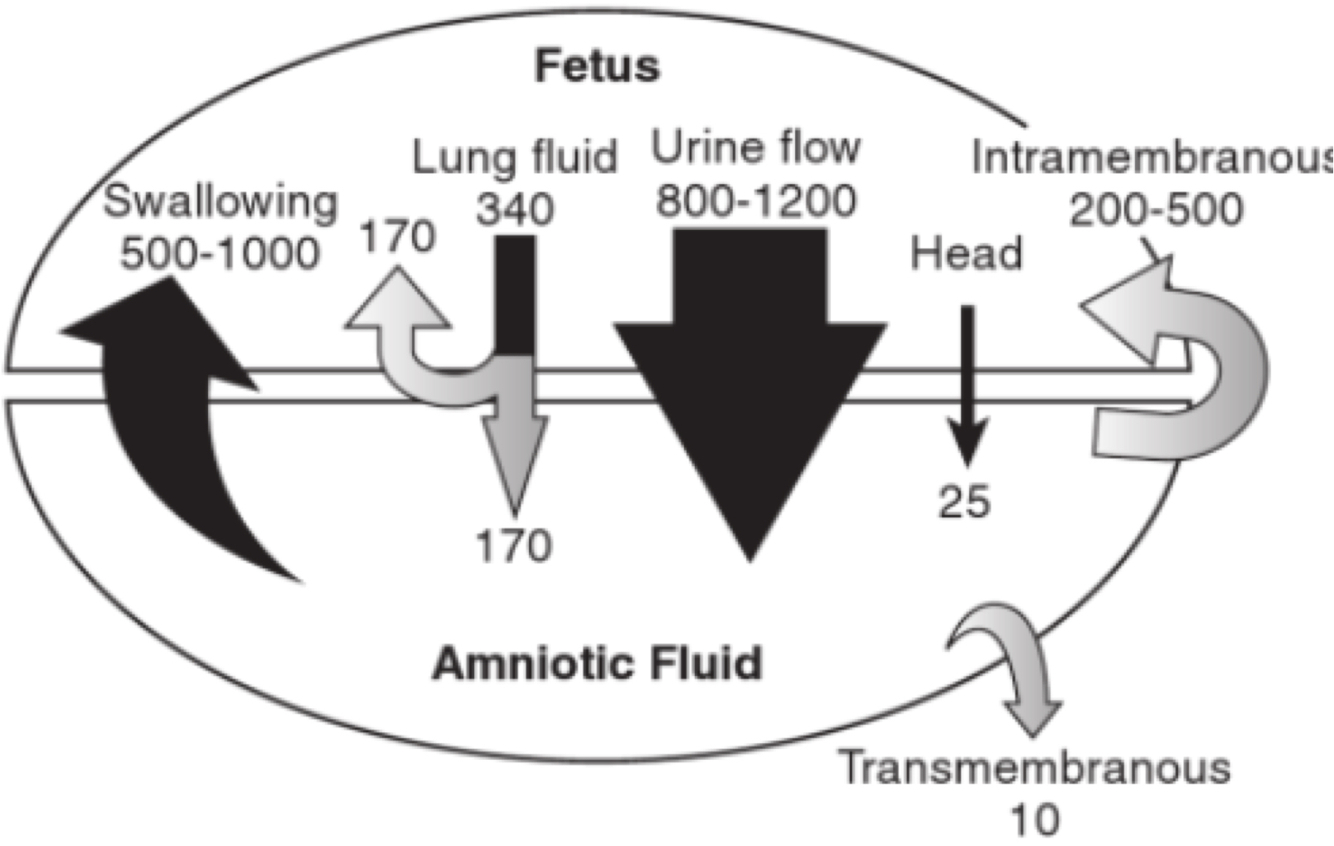
Amniotic fluid (amniotic sac encloses embryo / fetus in amniotic fluid)
- Function?
- Volume?
- How is it produced & recycled?
- Protection
- contributes to development of lungs
- Protection
- – 10 ml at 8 weeks
– Approx 1 litre at 38 weeks
– Falls away post-EDD
- • Fetal urinary tract (urine production by 9 weeks, up to 800 ml/day in T3)
- Fetal lungs
- Fetal GI tract
- Placenta and fetal membranes (intramembranous pathway)
- Composition of amniotic fluid
- What do we do with the amniotic fluid we remove in amniocentesis
- Bilirubin metabolism
- • 98% water
• Plus electrolytes, creatinine, urea, bile pigments, renin, glucose, hormones and fetal cells, lanugo and vernix caseosa
(• Swallowed
- Absorbs water and electrolyes
- Debris accumulates in gut – Meconium, debris from AF plus intestinal secretions including bile)
- Fetal cells useful diagnostic test – E.g. fetal karotyping
- • During gestation clearance of fetal bilirubin is handled efficiently by the placenta
- Fetus cannot conjugate bilirubin
- Immaturity of liver and intestinal processes for metabolism, conjugation and excretion
- Physiological jaundice common
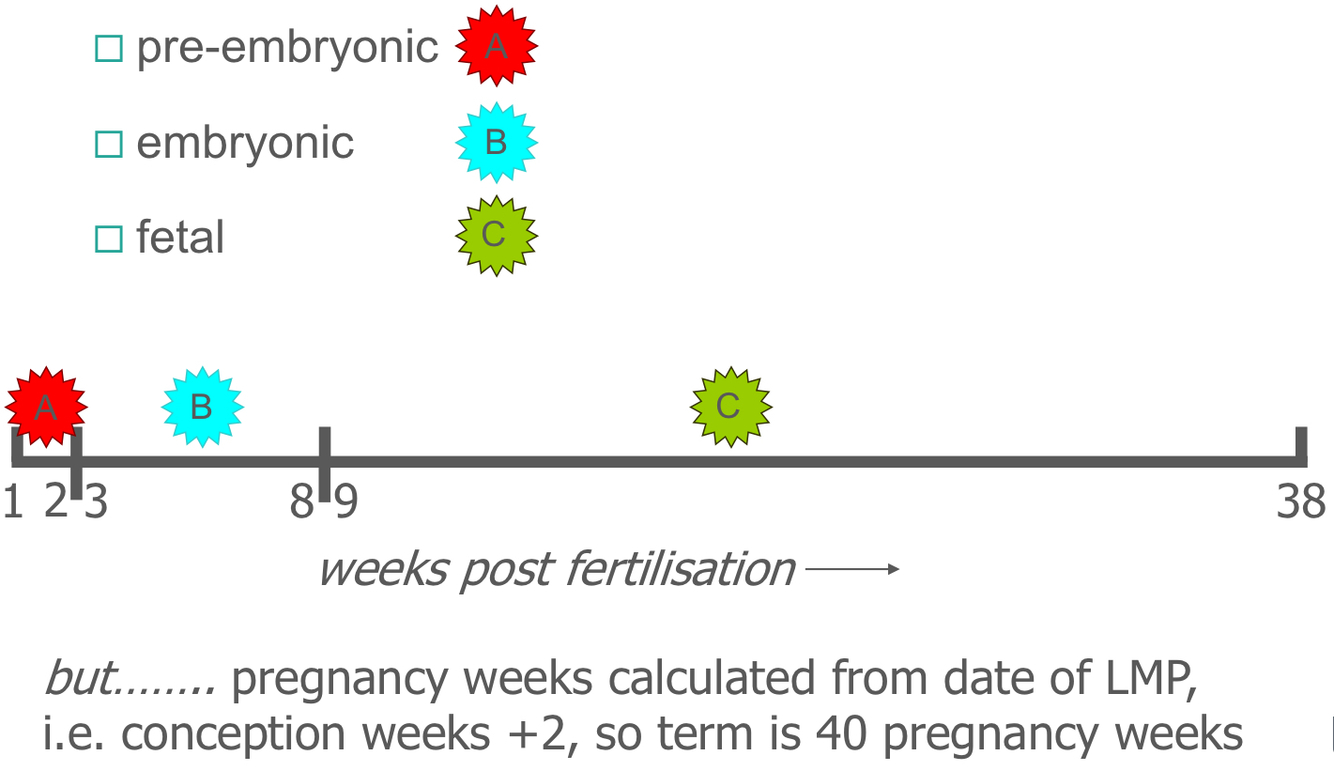
- Define the fetal period
- Define the pre- embryonic, embryonic and fetal periods using weeks
- • Growth and physiological maturation of the structures created during the (v much shorter) embryonic period
• Period involving preparation for the transition to independent life after birth
- image
• Embryonic period is characterised by intense activity
– organogenetic period
• But absolute growth is very small
– except placenta!
• Growth & weight gain accelerate in fetal period
Q. Draw a diagrammatic representation of patterns of growth during development (I.e. change in weight & height)
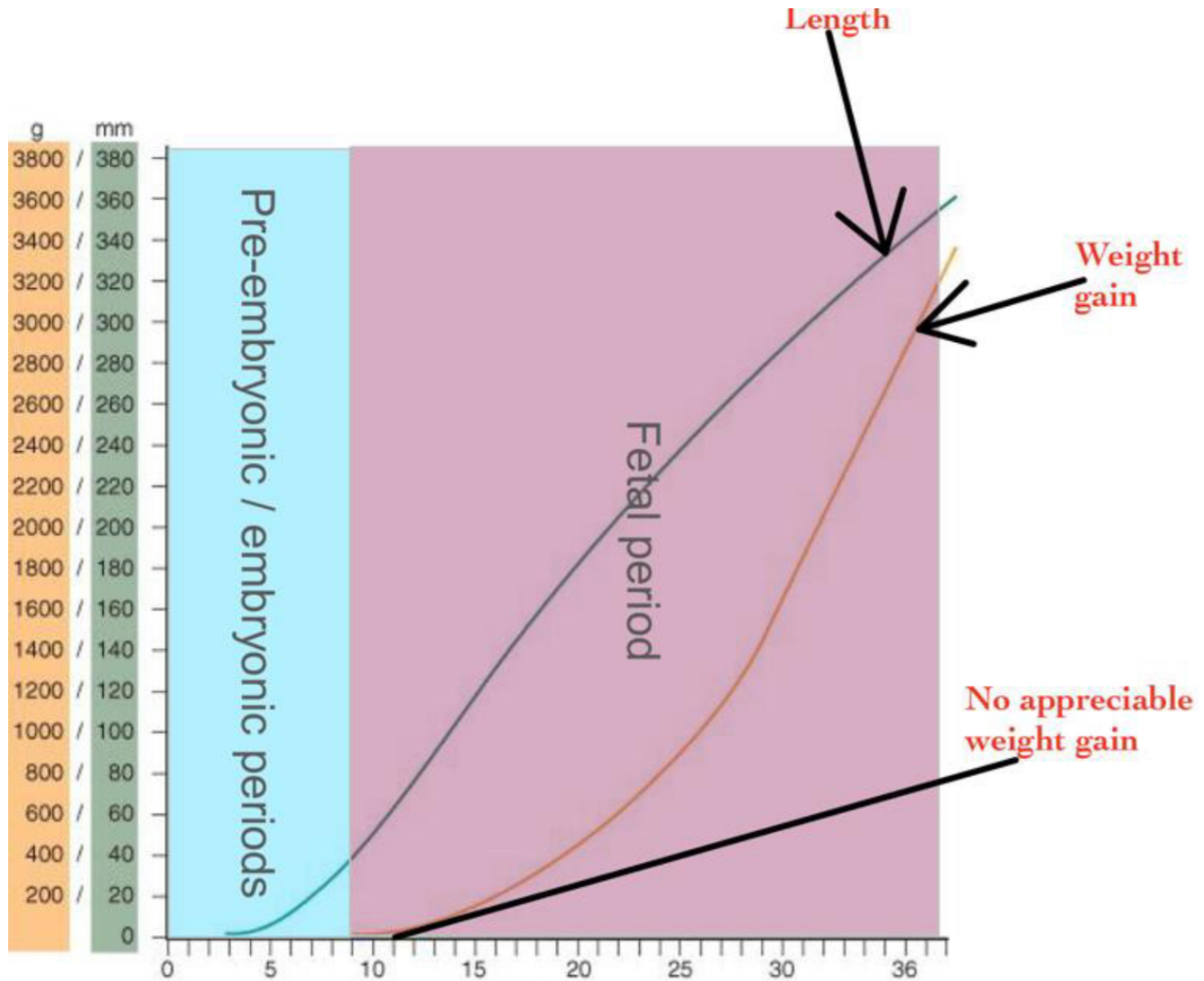
What is this diagram showing?
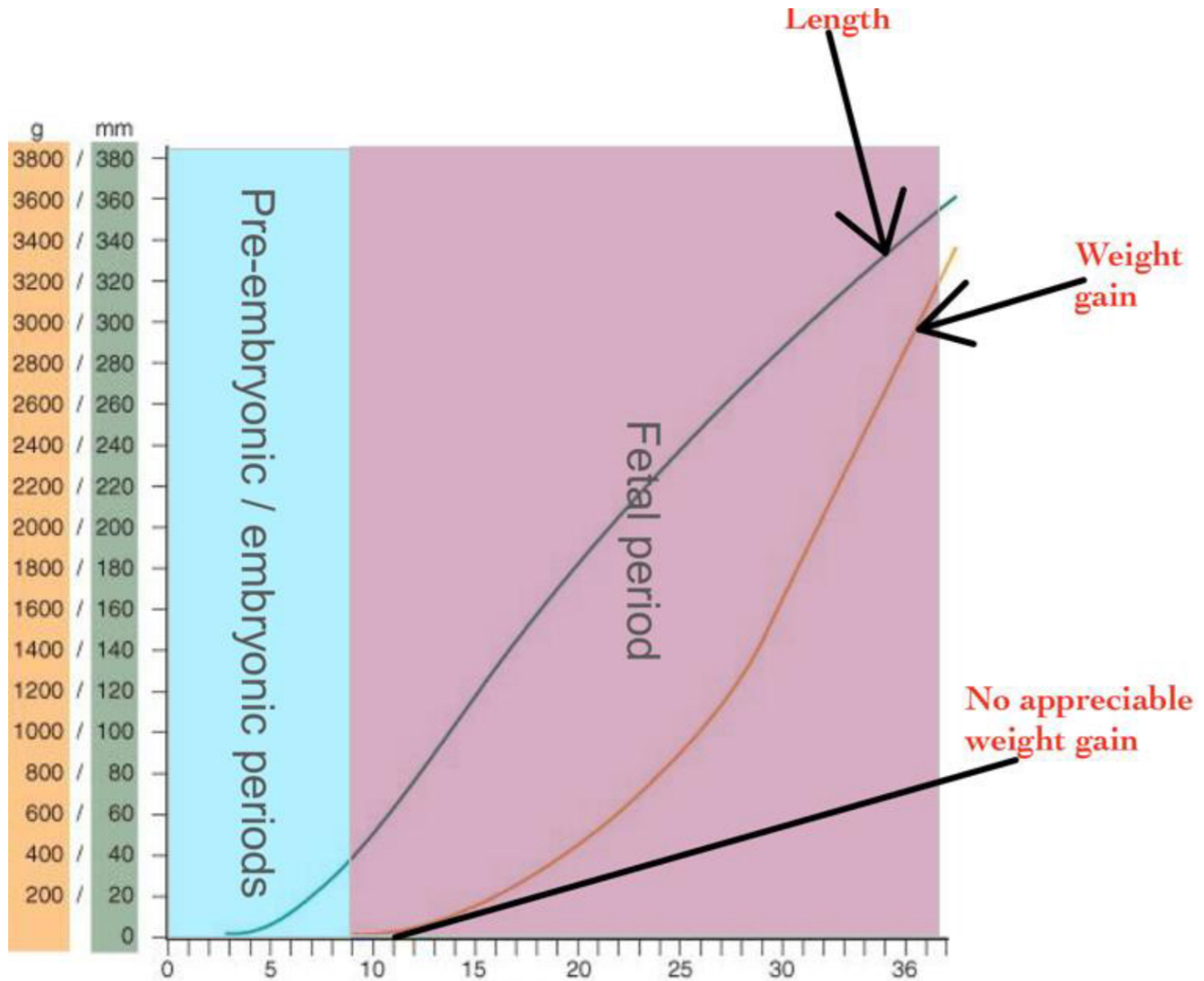
Embryonic period:
organogenetic period (formation & development of organs, intense morphogenesis & differentiation)
but absolute growth is very small except placenta!
Weight gain is slow
Fetal period:
Growth & weight gain accelerate
– Early fetus – protein deposition
– Late fetus – adipose deposition
- CRL increases rapidly in the pre-embryonic, embryonic & early fetal period
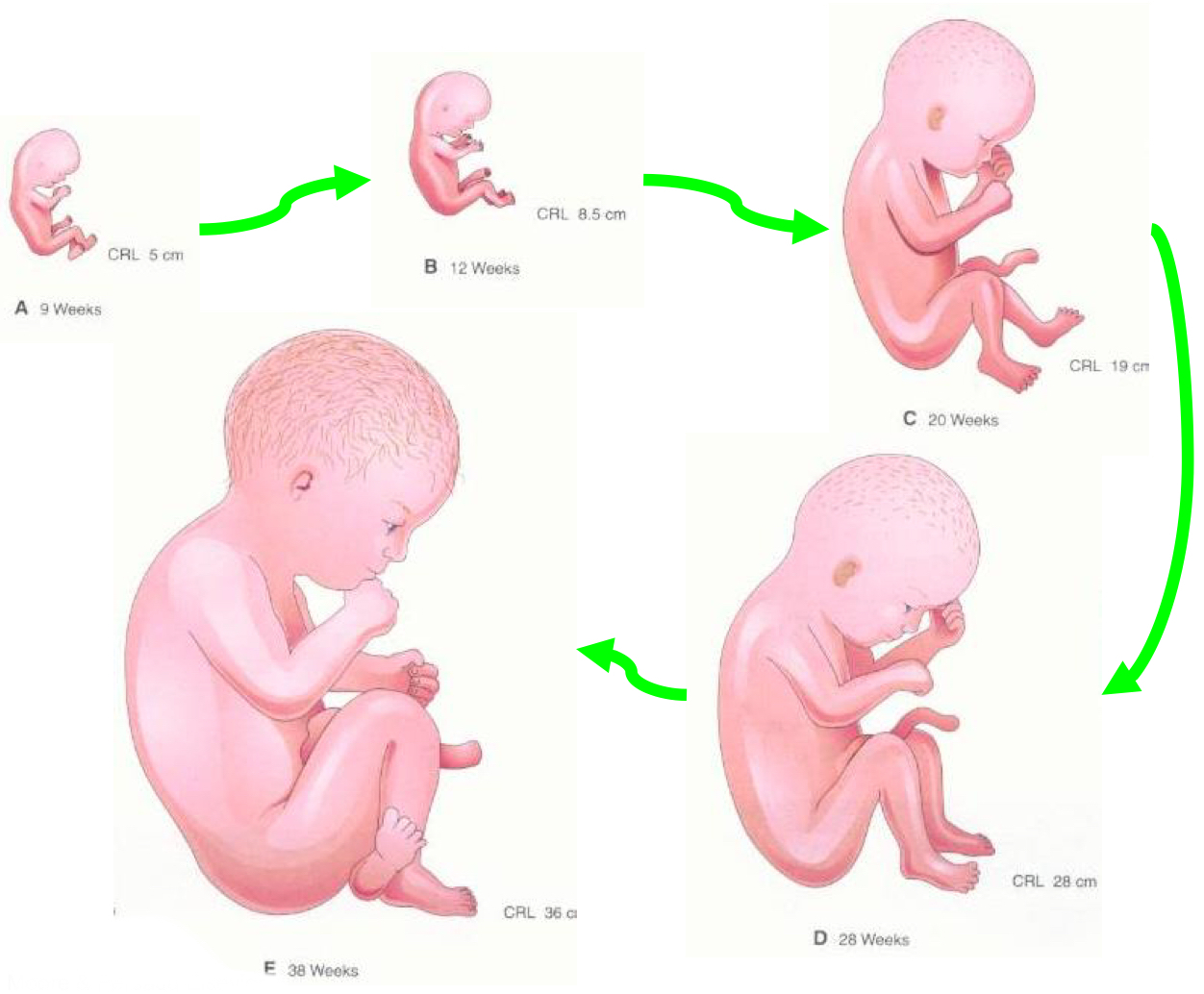
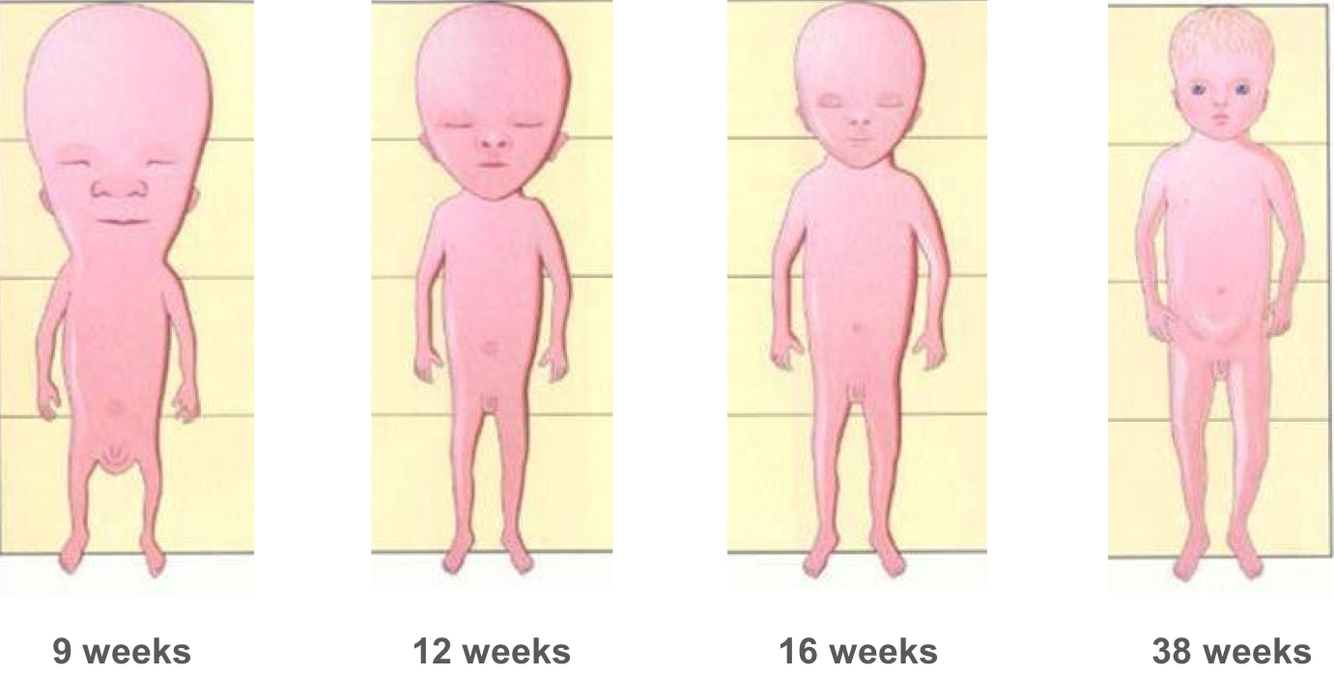
- Body proportions change dramatically during the fetal period, explain this statement.
- – at 9 week, the head is approx half crown-rump length
– thereafter, body length & lower limb growth accelerates
- Ante-natal assessment of fetal well-being:
- Estimation of fetal age
- • Mother -> Fetal movements
- Regular measurements of uterine expansion -> symphysis-fundal height
- Ultrasound scan ~20 weeks (calculate age,rule out ectopic, number of fetus, assess fetal growth, fetal anomalies)
- USS
• LMP
– Prone to inaccuracy
• Developmental criteria
– Allow accurate estimation of fetal age
What is measured in the first trimester?
Second & third trimester?
Crown-rump length (CRL)
- Measured between 7 & 13 weeks to date the pregnancy and estimate EDD
- Scan in T1 also used to check location, number, viability
Biparietal diameter
Used to date pregnancies in T2 & T3
Abdominal circumference & femur length
Dating & growth monitorin
Anomaly detection
- Classification of birth-weights
- 3500 g is considered average
- < 2500 g suggests growth restriction
- > 4500 g is macrosomia
– maternal diabetes
• Many factors influence birth weight, not all pathological
The importance of accurate dating
- Babies can have low birth-weight because –
- Respiratory system - late lung development
- premature
OR
constitutionally small
OR
suffered growth restriction
- – Embryonic development creates only the bronchopulmonary tree
– Fetal: Functional specialisation -> Major implications for pre-term survival
Describe the stages of the development of the respiratory system
Weeks 8 – 16: Pseudoglandular stage
• Duct system begins to form within the bronchopulmonary segments created during the embryonic period
– bronchioles
Weeks 16 – 26: canalicular stage
• Formation of respiratory bronchioles
– Budding from bronchioles formed during the pseudoglandular stage
Weeks 26 – term: terminal sac stage
• Terminal sacs begin to bud from the respiratory bronchioles
• Differentiation of Type I & Type II pneumocytes (surfactant)
The lungs during T2 & T3
- Where does gas exchange take place?
- How do the lungs prepare for gas exchange?
- Placenta
- • breathing movements
– conditioning of the respiratory musculature (otherwise atrophy of muscles)
• Fluid filled
– crucial for normal lung development (amniotic fluid has factors -> promote development of Type 1 & Type 2 pneumocytes -> surfactant)
Implications for pre-term survival
- Viability is only a possibility once the lungs have entered the terminal sac stage of development – i.e. ? weeks
- What is respiratory distress syndrome
- 24
- • Insufficientsurfactantproduction
• If pre-term delivery is unavoidable or inevitable
– glucocorticoid treatment (of the mother)
– increases surfactant production in fetus
- The definitive fetal H/R is achieved at around ? weeks – fetal bradycardia is associated with fetal demise
- Urinary system
• Fetalkidneyfunctionbeginsin week10
• Fetal urine is a major contributor to amniotic fluid volume
• Fetal kidney function is not necessary for survival in utero, but without it there is ?
- 15 (T2)
- oligohydramnios
- What terms do we use to little and too much amniotic fluid? Causes of each?
- Nervous system (first to begin development and last to finish)
When do our corticospinal tracts develop?
- • Oligohydramnios (too little)
– Placental insufficiency, fetal renal impairment
• Polyhydramnios (too much)
– Fetal abnormality – e.g. inability to swallow
- • Corticospinal tracts = 4th month
• Myelination of brain only begins in 9th month
– e.g. corticospinal tract myelination incomplete at birth, as evidence by increasing infant mobility in the 1st year
- What is Oligohydramnios?
- What is Polyhydramnios?
Causes? (3)
- Meaning of atresia
- Abnormalities include:
- – Too little
– Placental insufficiency, fetal renal impairment (all systems suboptimal)
The common clinical features are smaller symphysis fundal height, fetal malpresentation, undue prominence of fetal parts and reduced amount of amniotic fluid. - – Too much
– Fetal abnormality – e.g. inability to swallow
A single case: intrauterine infection (TORCH), rh-isoimmunisation, or chorioangioma of the placenta.
Multiple gestation pregnancy: twin-to-twin transfusion syndrome
Maternal: cardiac problems, kidney problems, and maternal diabetes mellitus, which causes fetal hyperglycemia and resulting polyuria (fetal urine is a major source of amniotic fluid). - an orifice or passage in the body is (usually abnormally) closed or absent
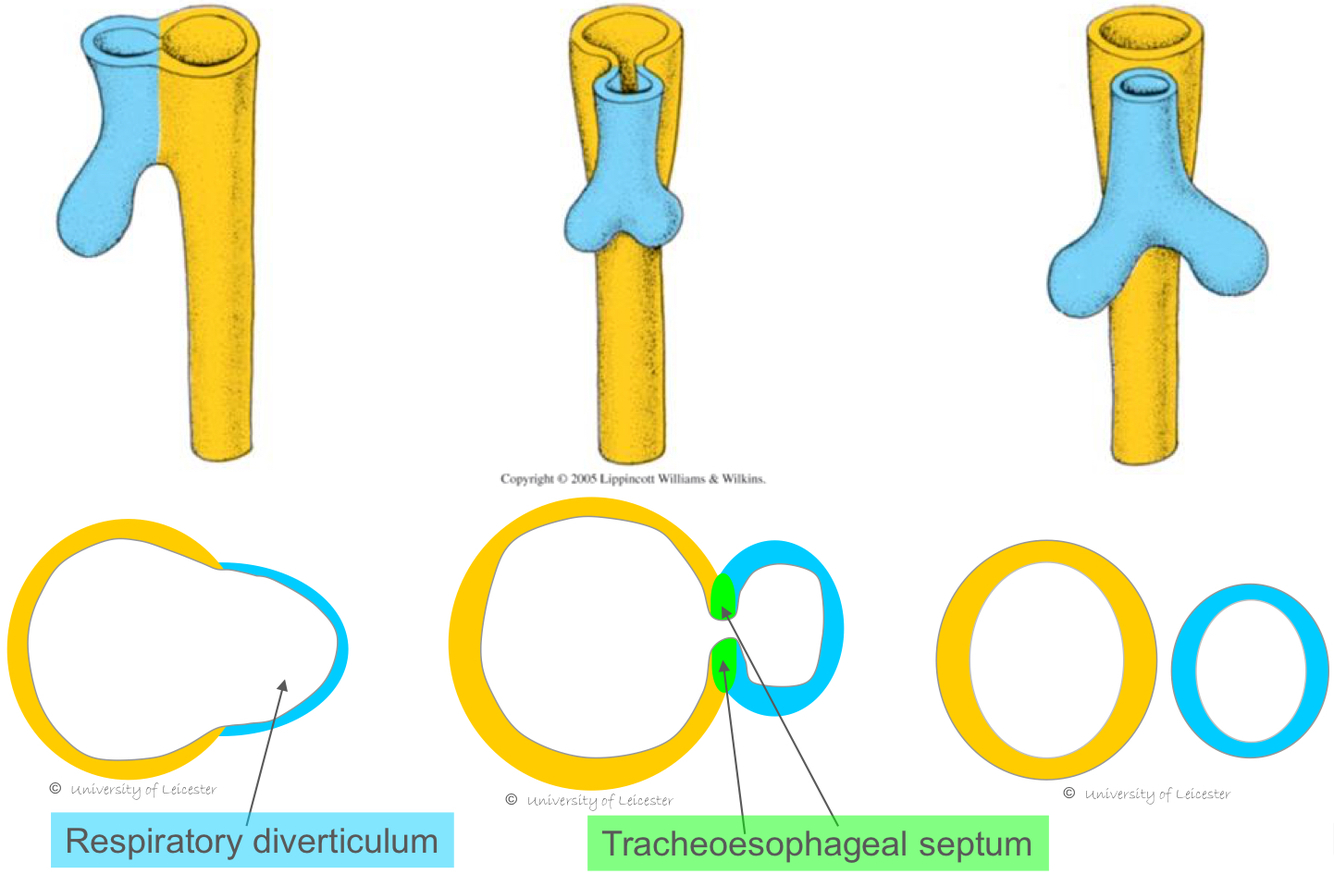
- Oesophageal atresia
- neurological abnormalities such as anencephaly, which impair the swallowing reflex. Anencephaly is failure of close of the rostral neuropore (rostral neural tube defect). If the rostral neuropore fails to close there will be no neural mechanism for swallowing.
- tracheoesophageal fistula
Sensory & motor systems
- No movement until the ?
- Thereafter a large repertoire of movements develop why? Give examples of some movements
8th week
practising for post-natal life
e.g. suckling, breathing
What is quickening?


