What is meant by ‘Shock’?
Used to describe acute circulatory failure with either inadequate or inappropriately distributed tissue perfusion, resulting in generalised lack of oxygen supply to cells.
How might inadequate tissue perfusion come about?
- Acute condition of inadequate blood flow throughout the body*
- A catastrophic fall in arterial blood pressure leads to circulatory shock*
- Cardiogenic shock: inability og the heart to eject enough blood e.g. in ischaemic cardiac damage
- Mechanical shock: due to a restriction on the filling of the heart e.g. cardiac tamponade, or obstruction to blood flow through the lungs e.g. pulmonary embolism
- Hypovolaemic shock: due to loss of circulating fluid volume (e.g. haemorrhage)
- Normovolaemic (distributive) shock: due to uncontrolled falls in peripheral resistance (e.g. in sepsis of anaphylaxis)
What could poor regional perfusion be due to?
Arterial occlusion: peripheral artery disease, coronary artery disease
Venous congestion: varicose veins, deep vein thrombosis
Describe Peripheral Vascular Disease in Veins
Veins contain ~70% if blood volume at any one time
Capacitance vessels have thin walls, low pressure, valves which prevent wrong direction of flow, external compression by skeletal muscle – musculovenous pump
Superficial vessels drain into deep vessels via perforating veins. If valves are incompetent, blood can go from deep veins to superficial veins –> varicose veins
Explain about Deep Vein Thrombosis
Commonly occur in calf veins, popliteal, femoral, iliac
Tender swollen calves
Risk of pulmonary embolism – chest pain, breathlessness
If there is a large PE resulting in occlusion, that can cause shock
What are varicose veins, and what can they lead to?
dilated, torturous superficial veins
Can be asymptomatic or lead to venous ulcers (chronic sores)
Explain about Coronary Artery Disease
atheromatous plaque, partially occluding coronary artery
Ischaemic heart disease
>70% occlusion – compromised blood flow when O2 demand increases and blood flow through LCA largely during diastole (shortens when HR increases –> limiting blood flow to LCA)
90% occlusion: ischaemia at rest
Discuss Ischaemic Heart Disease - Angina
Central chest pain – radiates to neck and left arm
Brought on by exercise, relieved by rest (stable angina)
Investigated with exercise stress test: 12-lead ECG, heart rate and blood pressure monitored whilst patient exercises on treadmill. Starts gently and increases in levels of exercise intensity
Test is positive if there is chest discomfort or ECG changes
Treatment: nitrates (main effect venodilation, reducing preload), β-blockers (reducing workload – contracts less hard, slower) and calcium channel antagonists reduce workload
Explain about Unstable Angina
Rapid onset pain at rest: severe central – radiates less
Disruption of atherosclerotic plaque and thrombus formation
Limited duration and extent of obstruction
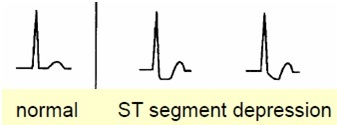
May be ST depression and/or T wave inversion
No detectable necrosis (cardiac enzymes and troponin not elevated)
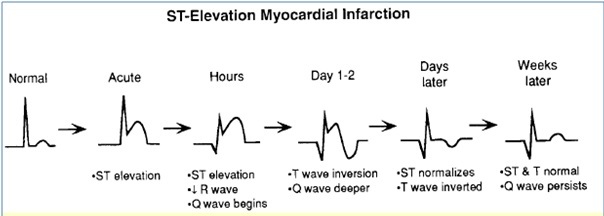
Explain about a STEMI
Acute severe central chest pain (crushing)
Radiating to neck, left shoulder and arm
Not relieved by rest
Be aware some patients do not experience pain
Strong sympathetic reaction: sweating, pallor due to sympathetic vasoconstriction
Rupture of atheromatous plaque – formation of thrombus (inappropriate clot: thrombus detaches or propagates along coronary artery and blocks it. Necrosis (death) of myocardial tissue
STEMI necrosis of full thickness of myocardial wall
NSTEMI more limited – ST depression and inverted T waves
ECG changes are most obvious in leads viewing the damaged myocardium
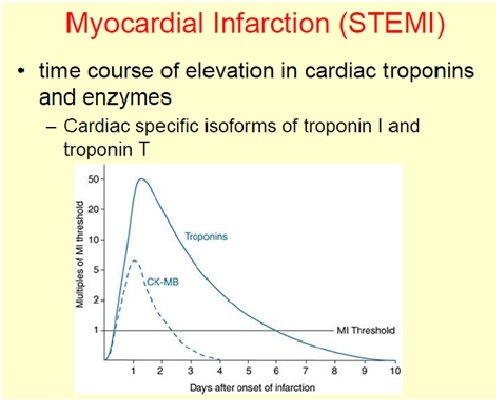
What biomarkers would you look for in a STEMI?
Specific cardiac troponin isoforms - TnI and TnT
Creatine Kinase MB
Explain about Cardiac Arrest
Unresponsiveness associated with lack of pulse
Heart has stopped or ceased to pump effectively
Asystole (loss of electrical and mechanical activity)
Ventricular fibrillation (uncoordinated electrical activity)
Most common form of cardiac arrest
May occur following MI or electrolyte imbalance or some arrhythmias (e.g. long QT and Torsades de Pointes)
Torsades de Pointes is a distinctive polymorphic ventricular tachycardia in which the QRS amplitude varies and the QRS complexes appear to twist around the baseline – associated with a prolonged QT interval, may degenerate into sustained ventricular tachycardia or ventricular fibrillation
Basic life support: chest compression and external ventilation
Advanced life support: defibrillation – electric current delivered to the heart, depolarises all the cells – puts them into refractory period. Allows coordinated electrical activity to restart
Adrenaline – enhances myocardial function, increases peripheral resistance
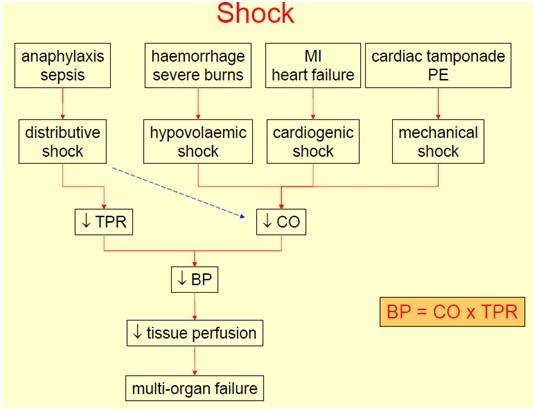
Essentially what can shock be due to?
Shock can be due to fall in CO or fall in TPR beyond capacity of the heart to cope
Fall in cardiac output could be due to mechanical (pump cannot fill), pump failure or loss of blood volume
- Cardiogenic shock (pump failure) – ventricle cannot empty properly
- Mechanical shock (obstructive) – ventricle cannot fill properly
- Hypovolaemic shock – reduce blood volume leads to poor venous return
Fall in peripheral resistance could be due to excessive vasodilation
Explain about Cardiogenic Shock
Acute failure of the heart to maintain cardiac output – pump failure
Following myocardial infarction: damage to left ventricle
Or due to serious arrhythmias (profound tachycardia orbradycardiaresulting in a drop in arterial pressure)
Acute worsening of heart failure
Central venous pressure (CVP) may be normal or raised; heart fills but fails to pump effectively
Dramatic drop in arterial BP
Tissues poorly perfused – coronary arteries which exacerbates problem, kidneys which leads to reduced urine production (oliguria) and brain which leads to loss of consciousness, confusion and dizziness
Explain about Mechanical Shock caused by Cardiac Tamponade
Blood or fluid build up in pericardial space (so heart is not able to expand)
Restricts filling of the heart – limits end diastolic volume
Affects left and right sides of heart
High central venous pressure
Low arterial blood pressure (ventricles can’t fill properly – not able to pump properly)
Heart attempts to beat – continued electrical activity
Explain about Mechanical Shock caused by Pulmonary Embolism
A massive pulmonary embolism occluding a large pulmonary artery could lead to circulatory shock
Pulmonary artery pressure is high
Right ventricle cannot empty
Central venous pressure is higher
Reduced return of blood to left heart – due to occlusion of pulmonary artery
Limits filling of left heart
Left atrial pressure is low
Arterial blood pressure is low
Shock
Also chest pain, dyspnoea
Explain about Hypovolaemic Shock
Reduced blood volume
Most commonly due to haemorrhage
~5L in an average 75kg man
<20% of blood loss unlikely to cause shock
20-30% some signs of shock response
30-40% substantial decrease in mean arterial blood pressure and serious shock response
Severity of shock is related to amount and speed of blood loss – worse if blood loss is rapid (more likely to go into shock with a smaller amount of blood loss if loss is rapid)
When there is a haemorrhage, venous pressure falls, cardiac output falls (Starling’s Law), arterial pressure falls and this is detected by Baroreceptors.
The compensatory response is increased sympathetic stimulation, tachycardia, increased force of contraction (due to increased contractility), peripheral vasoconstriction and venoconstriction (increases venous pressure –> increases return to heart)
Increased peripheral resistance due to peripheral vasoconstriction leads to internal transfusion, reducing the capillary hydrostatic pressure which increases THE NET MOVEMENT OF FLUID INTO THE CAPILLARIES.
Signs and symptoms of Hypovolaemic shock: tachycardia, weak pulse, pale skin and cold, clammy extremities
Apart from haemorrhage, hypovolaemic shock can also result from severe burns, severe diarrhoea or vomiting and loss of Na+
What can occur in Hypovolaemic Shock if treatment isn’t given?
Decompensation can occur if treatment isn’t given
Peripheral vasoconstriction (shutdown) impairs tissue perfusion
Tissue damage due to hypoxia
Release of chemical mediators – vasodilators which overcome sympathetic vasoconstriction effect
TPR falls
Blood pressure falls dramatically
Vital organs can no longer be perfused
Multi-system failure
Explain about Distributive Shock
Low resistance shock (normovolaemic – no change in blood volume); shock occurs because of fall in TPR
Profound peripheral vasodilation results in a catastrophic drop in TPR. Blood volume is constant but volume of the circulation has increased
Toxic shock
Anaphylactic shock
Explain about Toxic Shock
Septicaemia
Endotoxins released by circulating bacteria cause:
Profound vasodilation
Dramatic fall in TPR
Fall in arterial pressure
Impaired perfusion of vital organs
Also – capillaries become leaky but which reduces blood volume
Decreased arterial pressure: detected by Baroreceptors leading to increased sympathetic output. Vasoconstrictor effect overridden by mediators of vasodilation. Heart rate and stroke volume increased
Patient has tachycardia and warm, red extremities because of vasodilation however later stages of toxic shock - vasoconstriction
Explain about Anaphylactic Shock
(severe allergic reaction – anaphylaxis)
Release of histamine from mast cells (and other mediators such as prostaglandins, leukotrienes and cytokines) has a powerful vasodilator effect – fall in TPR
This results in a massive drop in arterial pressure which via the baroreceptor reflux, leads to an increased sympathetic response – leading to increased CO but can’t overcome vasodilation
Impaired perfusion of vital organs
Mediators also cause bronchoconstriction and laryngeal oedema – difficulty breathing
Patient will have difficulty breathing, collapse, rapid heart rate and red, warm extremities
Acutely life-threatening
Treatment: adrenaline – vasoconstriction via action at α1 adrenoceptors – works on β2 normally to cause vasodilation but in high enough concentration binds to α1 adrenoceptors to cause vasoconstriction to try and increase venous return to the heart and therefore increase cardiac output
Give an overall summary of shock
Explain about Hypertension
sustained increased in arterial blood pressure
Arterial BP > 140/90 mmHg
BP = CO x TPR
CO = SV x HR
Regulation of blood pressure at three sites:
- Kidneys (regulates blood volume which alters SV)
- Heart regulates CO through altering rate and force of contraction
- Vasculature regulates TPR
What are the consequences of hypertension?
Long standing hypertension –> left ventricular hypertrophy (risk of heart failure)
Risk of arterial disease
- Coronary arteries – MI, angina
- Cerebrovascular system – stroke
- Renal vasculature – kidney failure
- Aorta
