Renal Physiology 2 Flashcards
Describe the renal mechanisms for excreting dilute urine.
- When there is a large excess of water in the body, the kidney can excrete as much as 20L/day of dilute urine, with a concentration as low as 50 mOsm/L in the absence of ADH.
- This is achieved by the kidney continuing to reabsorb solutes while failing to reabsorb large amounts of water in the distal parts of the nephron, including the late distal tubule and collecting ducts.
- When there is a deficit of water, the kidneys can excrete highly concentrated urine with an osmolarity of 1200-1400 mOsm/L.
- Note: the ability to regulate water excretion INDEPENDENTLY of solute excretion is necessary for survival, especially when fluid intake is limited.
Describe how the kidneys can control water excretion by changing [ions] in the nephron tubule.
- Normal osmolarity of the extracellular fluid is 300 mOsm/L when entering the kidney.
- This is REDUCED to ~100 mOsm/L by the time the filtrate enters the DCT due to the reabsorption of ions.
- This osmolarity is further reduced in the DCT and collecting ducts as there is addition reabsorption of NaCl.
- The failure to reabsorb water and continued reabsorption of ions leads to a large volume of dilute urine.

Describe the state of tubular fluid in the proximal tubule.
- Tubular fluid remains isosmotic in the proximal tubule.
- As the filtrate flows through the proximal tubule, solutes and water are REABSORBED in equal proportions, so little change in osmolarity occurs.
- The proximal tubule fluid remains isosmotic to the plasma, with an osmolarity of ~300 mOsm/L.
- Water is reabsorbed by osmosis and the filtrate reaches equilibrium with the surrounding interstitial fluid of the renal medulla, which is very hypotonic.
- Thus, the filtrate becomes more concentrated as it flows into the inner medulla.
Describe the state of tubular fluid in the ascending loop of Henle.
- In the ascending limb, especially in the THICK segment, sodium, potassium and chloride are greatly reabsorbed.
- The ascending limb is impermeable to water, EVEN in the presence of large amounts of ADH.
- Thus, the filtrate becomes more DILUTE as it flows up the ascending limb into the early distal tubule - osmolarity ~100 mOsm/L.
- Filtrate leaving the early distal tubular segment is hypo-osmotic with an osmolarity of ~1/3 of the osmolarity of plasma.
Describe the state of tubular fluid in the distal and collecting tubules in the absence of ADH.
- As the dilute filtrate in the early distal tubule passes into the LATE distal convoluted tubule → cortical collecting duct → and collecting duct → there is additional reabsorption of NaCl.
- In the absence of ADH this portion of the tubule is also impermeable to water.
- Additional reabsorption of solutes causes the filtrate to become even more dilute, decreasing its osmolarity to as low as 50 mOsm/L.
Describe how the kidneys make and excrete urine that is more concentrated than plasma.
- The ability to make and EXCRETE urine that is MORE concentrated than plasma is essential for survival.
- This allows conservation of water, especially when water intake is limited.
- Human kidney can make urine up to a maximum of 1200-1400 mOsm/L → 3-4 times that of the plasma.
- There needs to be a high level of ADH that allows the DISTAL tubules and collecting ducts to become permeable to water and so reabsorb water.
- There also needs to be a gradient to PULL this water out from the filtrate → there is a high osmolarity of the renal medullary interstitial fluid
- Renal medullary interstitium surrounding the collecting ducts is normally hyperosmotic → when ADH levels are high → water moves through the tubular membrane by osmosis into the renal interstitium → the water is then carried away by the vasa recta back into the blood.
What are the major factors which contribute to the build-up of [solute] into the renal medulla?
- ACTIVE transport of sodium ions and co-transport of potassium, chloride, and other ions OUT of the thick portion of the ascending limb INTO the medullary interstitium.
- ACTIVE transport of ions from the collecting ducts INTO the medullary interstitium.
- FACILITATED diffusion of urea from the inner medullary collecting ducts into the medullary interstitium.
- Diffusion of only small amounts of water FROM the medullary tubules into the medullary interstitium.
- FAR LESS than the reabsorption of solutes into the medullary interstitium.
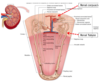
Give an overview of the movement of ions and water throughout the nephron.

What are the special characteristics of the loop of Henle that cause trapping of solutes in medulla?
- A major reason for the high medullary osmolarity is ACTIVE transportof sodium and co-transport of K+, Cl- and other ions from the THICK ASCENDING loop into the interstitium.
- This pump is capable of establishing [~200 mOsm] gradient between the tubular lumen and the interstitial fluid.
- Remember - the thick ascending limb is impermeable to water, the solutes pumped out are not followed by osmotic flow of water into the interstitium.
- Thus, the active transport of sodium and other ions out of the thick ascending loop adds solutes in EXCESS of water to the renal medullary interstitium.
- Some passive reabsorption of sodium chloride from the THIN ascending limb, which is also impermeable to water, adding further to the high [solute] if the renal medullary interstitium.
- Remember, the descending limb is VERY permeable to water - the tubular filtrate osmolarity quickly becomes EQUAL to the renal medullary osmolarity.
- Note - the vasa recta flow is in the opposite direction to the filtrate flow in the loop of henle → counter-current and establishes a concentration gradient for solutes and an osmotic gradient.
Describe the action of the loop of Henle tubular counter-current mechanism.
- The loop of Henle tubular counter-current multiplier actively generates a concentration gradient that is greater the deeper into the medulla you go.
- Step 1: filtrate enters the loop from the PCT at 300 mOsm/L - the same as plasma.
-
Step 2: Active transport of ions from the THICK ascending (impermeable to water) limb establishes a 200 mOsm/L gradient between the filtrate and the interstitial fluid.
- 400 mOsm/L in the medullary interstitium compared to 200 mOsm/L in the ascending tubule fluid.
-
Step 3: the filtrate in the descending limb (permeable to water, but impermeable to salt) now equilibrates with the interstitial fluid → water moves down its osmotic gradient into the medulla interstitial fluid.
- Continued transport of ions, but NOT WATER in the ascending limb maintains the gradient.
-
Step 4: Flow of fluid into the loop of Henle from the PCT MOVES the filtrate in the limbs onwards.
- The hyperosmotic (highly concentrated) filtrate in the descending limb MOVES on into the ascending limb.
-
Step 5: This hyperosmotic filtrate that enters the ascending limb then has additional ions (passive at thin and active at thick) pumped out until a 200 mOsm/L gradient is AGAIN established between the ascending tubule fluid and the medullary interstitium.
- This time the interstitial osmolarity rises to 500 mOsm/L and the ascending filtrate falls to 300 mOsm/L (at the top of ascending).
-
Step 6: there is again movement of water OUT OF the descending limb to reach osmotic equilibriumwith the medullary interstitial fluid.
- This increases the osmolarity of the tubule fluid in the descending UP TO 500 mOsm/L which moves on into the ascending limb for sodium and other ion movement from the filtrate into the medullary interstitium.
- These steps are repeated over and over - the net effect of adding more and more solute to the medulla in EXCESS of water.
- This process gradually TRAPS solutes in the medulla and MULTIPLIES the concentration gradient established by the active pumping of ions out of the THICK ASCENDING loop of Henle, eventually raising the interstitial fluid osmolarity to 1200-1400 mOsm/L.
- THUS, the repetitive reabsorption of NaCl from the thick ascending loop and CONTINUED inflow of NEW NaCl from the proximal tubule into the loop is called the countercurrent multiplier.
- The NaCl reabsorbed from the ascending loop of Henle keeps adding to the NEWLY ARRIVED NaCl, thus “multiplying” its concentration in the medullary interstitium.

Describe the formation of concentrated urine.
- Tubular fluid LEAVING the loop into the DCT is ~100 mOsm/L.
- The DCT continues to REMOVE ions due to ACTIVE transport of NaCl and so the osmolarity of the filtrate continues to FALL.
- In the cortical section of the collecting ducts the amount of water that is reabsorbed from this dilute urine is dependent on ADH levels.
- Presence of ADH → the absorbed water is rapidly transported OUT of the kidney by the large blood flow through the kidney cortical peritubular capillaries.
- This water absorption in the KIDNEY CORTEX rather than the medulla helps to preserve the osmotic gradient (hyperosmotic) in the MEDULLA.
- As the fluid continues through the collecting duct and through the medulla, there is MORE water reabsorption into the medullary interstitium.
- This is a small volume of water reabsorption in comparison to the kidney cortical region, and this water in the medulla is carried AWAY by the vasa recta into the venous supply.
- High levels of ADH - the collecting ducts become more permeable to water and the filtrate at the end of the collecting ducts is the same osmolarity as the renal medulla ~1200 mOsm/L.
- Thus, by reabsorbing as much water as possible the kidneys can produce a concentrated urine.
- Note - the filtrate leaving the loop of Henle is dilute, but becomes highly concentrated as water is absorbed from the distal tubules and collecting ducts.

How can urea be used to make concentrated urine?
- Urea can contribute to the osmolarity of the medullary interstitial gradient when the kidney needs to form MAXIMALLY concentrated urine in dehydration.
- Normally in PCT → 40-50% of the filtered urea is REABSORBED, but the [urea] in the tubular filtrate still increases as this reabsorption is LESS than that of water.
What happens to urea when there is a water deficit and ADH is high?
What happens in the descending limb?
- Large amounts of urea are PASSIVELY reabsorbed from the inner medullary collecting ducts into the interstitium.
- In the descending limb → the [urea] continues to RISE due to further water reabsorption into the medullary interstitium and the movement of urea from the medullary interstitial fluid BACK INTO the tubule.
- Both passive and ACTIVE secretion.
What effect does urea have on the sections of the nephron in the cortical region?
- The sections of the nephron in the cortical region → the thick ascending, the DCT and the cortical collecting ducts are all relatively impermeable to urea → urea DOES NOT move back into the tubule fluid.
- The presence of ADH and the further reabsorption of water from these cortical tubule sections results in further INCREASES in the [urea] of the urea already in the tubule.
- As the tubular filtrate move on into the medullary collecting ducts, even more water is absorbed and the urea becomes even more concentrated.
What happens as a result of high levels of urea in the tubular medullary collecting ducts?
- This high [urea] causes the urea to diffuse OUT of the medullary collecting duct into the medullary interstitial fluid.
- This is facilitated by specific urea transporters → one of these transporters is activated by ADH (water deficit) → enhancing the movement of urea OUT of the medullary collecting duct into the medullary interstitial fluid.
- A moderate amount of this urea can move BACK INTO the tubule at the inner medullary section of the loop of Henle → thus, the urea can recirculate through the tubule distal to this part of the nephron several times.
- This recirculation can contribute to the [urea] in the distal tubular fluids in times of dehydration.
- The urea recirculation provides an additional mechanism for the formation of the hyperosmotic renal medulla.
- In FULL HYDRATION where water is to be lost, tubular flow is GREATER and this recirculation of urea is LESS MARKED and contributes LESS.

Describe the blood flow through the vasa recta.
- The medullary blood flow is LOW → is ~5% of the total renal blood flow.
- This is enough to supply the metabolic needs of the tissues, but DOES NOT result in the loss of solute from the medullary interstitium.
- 2 special features of the renal medullary blood flow contribute to the preservation of the high [solute]:
- The low medullary blood flow is just enough to meet the metabolic needs → No loss of solute.
- The vasa recta serve as counter-current exchangers - minimising the washout of solutes from the medullary interstitium.
- Blood becomes more HYPERTONIC as it descends into the medullary interstitium and then becomes LESS hypertonic as it ascends back towards the cortical regions.
- Solutes and water move to mirror concentrations in the medulla.
- The vasa recta DO NOT CREATE the medullary hyperosmolarity, but they prevent it from being dissipated.
- Note - increased medullary blood flow reduces the urine-concentrating ability. Certain vasodilators can markedly increase renal medullary blood flow - “washing out” some of the solutes from the renal medulla - reduces the maximum urine-concentrating ability.
- The U-shaped structure minimises loss of solute from the interstitium, but DOES NOT prevent the bulk flow of fluid and solutes into the blood through the usual colloid osmotic and hydrostatic pressures that FAVOUR reabsorption in these capillaries.

What is caused by an increase in extracellular fluid osmolarity (increase in plasma [Na+])?
- Causes nerve cells (osmoreceptors) located in the anterior hypothalamus near the supraoptic nuclei to shrink.
- Shrinkage of the osmoreceptor cells causes them to FIRE → sending nerve signals to additional nerve cells in the supraoptic nuclei, which then relay these signals down to the stalk of the pituitary gland to the posterior pituitary.
- These action potentials conducted to the posterior pituitary stimulate the release of ADH → ADH is stored in the secretory granules in the nerve endings.
Where is ADH stored?
Secretory granules in the nerve endings.
What happens to ADH once it has entered the blood stream?
What effect does it have?
- Once ADH has entered the bloodstream, it is transported to the kidneys:
- It increases the water permeability of the late distal tubules, cortical collecting tubules and the medullary collecting ducts.
- The increased water permeability in the distal nephron segments causes INCREASED water reabsorption and EXCRETION of a small volume.
- Thus, water is conserved in the body while sodium and other solutes continue to be EXCRETED in the urine.
- This causes dilution of the solutes in the extracellular fluid, thereby correcting the initial excessively concentrated extracellular fluid.

